Health Care and Natural Ventilation



In a way, though, the XiangYa design team is fighting with one hand tied behind its back: while the client’s mandate calls for natural ventilation and cooling, it also calls for a building envelope primarily of glass. “It’s an unfortunate trend,” says Menchaca. “The more solar gain we have in a space, the larger the opening needs to be to vent it.” Payette’s in-house research had established that windows opening 4 inches (the maximum allowed for safety) could be configured as louvers, or as high and low awning windows, to achieve a significant increase in the number of air changes per hour compared to a casement window of the same size. But the ventilation needs of XiangYa’s glassy spaces outstrip what any type of 4-inch opening can provide.

IMAGES: COURTESY PAYETTE
QUIET CORNER
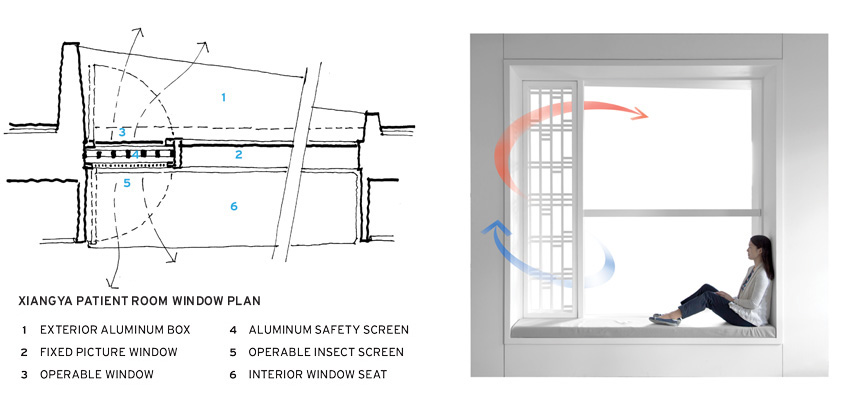
The design for Fifth XiangYa Hospital in Changsha, China (top), includes operable windows (bottom, left and right) that rely on the stack effect to ventilate the patient rooms. The windows incorporate patterned screens, shading devices, and a bench.
Payette’s solution is to provide for safety and ventilation separately. A patterned aluminum screen, with openings sized to comply with the 4-inch safety maximum, will serve as a guard on the interior side of the window. This will free the window, sized tall enough to generate a stack effect, to open fully. The assembly will form part of a window frame and seat in each patient room. Outside, the frame projects to act as a shading device for the glass. For the patient, the window will provide fresh air and views to gardens, while the scale of the window box will offer a sense of intimacy in the large building. “It would be a hard sell in the U.S.,” says Menchaca. “Who’s going to clean the screen? Who’s going to open the window?” But for a client already used to operable windows and insect screens, these concerns don’t arise. Even so, Payette has designed the insect screen to swing inward for ease of cleaning both sides.
NTFGH and XiangYa are just two among many instances of naturally ventilated health-care facilities internationally, but North American examples are few and far between. A survey conducted by Payette of health-care architects, engineers, and owners in the U.S. suggests that the industry’s main concerns pertain to a perceived lack of infection control, the logistics of controllability, patient comfort, and added construction costs. Perceived advantages include a connection to the outdoors, resilience in the event of power failure, improved working conditions and patient care, and reduced operating costs.
Infection control is highest on the list of cited concerns. But proponents of natural ventilation in health-care environments say that these worries are based on a misunderstanding of where natural ventilation will be used. Certain areas are generally considered inappropriate for it, including operating rooms, the sterile core, procedure suites, interventional radiology and cardiology areas, airborne isolation rooms (unless separately exhausted), protective environments, and intensive care units. Outside the operating room, the most common hospital-acquired infections (HAI) are pneumonia, urinary tract, bloodstream, and gastrointestinal diseases, none of which are likely to be affected by ventilation systems. In fact, HAI rates in Europe, where natural ventilation is common, are no higher than those in the U.S.
Peace Island Medical Center, the 39,000-square-foot, two-story facility in Washington State, exemplifies North America’s baby-steps approach. Located in a climate where mild summers make natural ventilation a perfect fit, the facility, which opened in 2013, is “a very modest starter kit,” says Anne Schopf, partner and director of design at Seattle-based Mahlum Architects. “The accomplishment was huge, but the risk was also lower because of climate and project scale.”
With a goal of resilient health-care delivery on an island where power outages are common, the design team tailored the hospital’s environmental control systems to its program areas’ specific needs. In inpatient areas, which are intermittently or partially occupied, operable windows provide cooling and ventilation (supplemental fans prevent air changes from falling below code minimums); the outpatient clinic, which accounts for about a third of the building, uses the same setup as the inpatient areas, but with a more basic fan exhaust providing fewer air changes. Emergency and imaging departments are conditioned by mechanical means using a conventional variable air volume (VAV) system and ground-source heat pumps; the surgery is equipped with a dedicated fan-coil unit that can be shut down when the space is not in use. This design has enabled Peace Island to achieve an EUI of 87.7 kBtu per square foot per year (a typical hospital in the Pacific Northwest scores around 265).
After more than four years of operation, “I’d say the majority of users think [natural ventilation] is great,” says Ben Coon, regional construction project manager for PeaceHealth. But with only two or three inpatients admitted per day, he adds, the data pool is tiny.
Even for so small a facility in an ideal climate zone, however, obtaining Department of Health approval for operable windows wasn’t easy. Concerns included humidity, security, pollen and dust, infection control, staff controls, patient experience, and the durability of interior materials. Ultimately, PeaceHealth provided reassurance in the form of a memorandum, included with its building-permit application, describing the design provisions and operating policies by which each DoH-identified concern would be addressed.


PHOTOGRAPHY: © BENJAMIN BENSCHNEIDER
STARTER KIT
The modest scale of the Peace Island Medical Center (top and bottom) in Washington State, along with the Pacific Northwest climate, made it the perfect candidate for natural ventilation.
“It comes down to liability,” says Coon, and, with operable windows an ideal rather than a necessity, “We probably would have given up.” But the design team persevered, and today the Peace Island Medical Center stands as a path-breaking solution for its circumstances.
That path may be about to open up. At this year’s ASHRAE annual conference, in Long Beach, California, Travis English presented the natural-ventilation task group’s position paper summarizing its two-year review of ASHRAE Standard 170: Ventilation of Health Care Facilities. If a design culture of mechanical ventilation is what makes North Americans leery of adopting natural ventilation for health care, Standard 170, which a number of jurisdictions have incorporated into their building codes, is what locks that design culture into industry practice. The standard’s provision that “all of the air provided to a space shall be filtered” and that “the entire minimum outdoor air changes per hour . . . shall meet the filtration requirements” may have been intended to apply only to mechanically supplied air, but Standard 170 is widely understood to preclude natural ventilation anywhere in a health-care facility.
The task group’s position paper calls for change, suggesting that natural ventilation should be allowed in most health-care spaces, except for operating rooms and other critical areas. Among the likely benefits, the paper identifies energy reduction and enhanced occupant satisfaction. It advises designers to fully consider space and climate appropriateness, acoustics, security, and outdoor air quality, and cautions that projects implementing natural ventilation should anticipate challenges, since many commissioning agents and air-balance providers in the United States are unfamiliar with natural-ventilation systems. “We’re going to look at that horse’s teeth pretty hard,” says English, speaking from a facility owner’s perspective, “but it should be something we have the choice to evaluate. It should be an option.”
Katharine Logan is a designer and writer focusing on design, sustainability, and well-being.
Notice



