Ease of Wayfinding and Circulation Cues
Wayfinding helps patients and visitors navigate a facility with minimal assistance and no confusion. Flooring color can identify room types and patterns to guide people toward their destination.
According to the VA design guide for behavioral and mental health facilities, “Design can support elements by using color to identify program areas. For example, a consistent color can identify all staff off-stage areas. Patient units can be identified by distinct and different color palettes. Group Rooms may be identified with consistent color.”31
FGI Guidelines speak to pattern and color contrast research. Patterns and contrast research suggest that flooring with a medium-sized pattern (1 to 6 inches wide, or 2.54 to 15.24 centimeters wide) was associated with more falls than floors with no design or a small pattern (less than 1 inch wide, or 2.54 centimeters wide), or a large pattern (wider than 6 inches). High-contrast patterns with large geometric or swirling designs on floor surfaces have been associated with more patient falls. These patterns can distract and potentially confuse persons with visual acuity issues.
Minimal Contrast Between Types of Flooring
In the United States, 8 percent of the population (26.M), and 1:5 who are over sixty-five are visually impaired. Similar values between different flooring materials help minimize transitions between different types of flooring and may reduce fall risk. Smooth transitions should be provided between different flooring materials. Flush thresholds should be used to reduce tripping hazards. Some flooring types, such as resilient flooring (e.g., rubber, luxury vinyl tile, sheet vinyl) and carpet, should include transition strips that minimize trip hazards.
Slip Resistance
The slip-resistance ratings of flooring surfaces should be appropriate for the area of use—for dry or wet conditions and use on ramps and slopes.
According to FGI 2022 Guidelines for Design & Construction of Hospitals: Wet conditions are common in areas such as kitchens and bathing areas, entries from exterior to interior space, and areas where water is used for patient services. Slip resistance is also an important consideration for ramps and stairways. In dry areas, soft flooring (e.g., carpet, cushioned flooring) can reduce the risk of falls and the impact of associated injuries.
Compatible with Wheeled Devices
Floor surfaces should allow easy movement of all wheeled equipment in the facility. Portable lifting equipment without powered wheels may require more exertion by staff than ceiling-mounted equipment to move an elevated patient around and through a space. The exertion required by staff may increase with the use of carpet; however, different types and brands of carpet may have significantly different levels of resistance to wheeled devices. Installation of a mock-up to test hybrid flooring materials with wheeled equipment and devices used in a facility is recommended. Carpet should not be automatically discounted as inappropriate due to this challenge, as it has significant advantages over hard-surface flooring in terms of noise reduction and acoustics.
Floor Reflectivity and Glare
Finished floors with a high gloss value cause glare that may compromise patient vision by being misinterpreted as a pool of water on the floor or a hole in the floor surface, disrupting the balance. The use of no floor finish flooring eliminates glare. Where a floor finish is required, smooth flooring surfaces should be sealed with a matte finish to reduce surface glare. A minimum LRV of 30 is recommended between floors and walls (wall bases should match the walls) to help define the space.
Sound Attenuation (Reduce Impact Sound)
Reducing impact sound requires specifying the right product for the right space. Acoustic floors should be selected with consideration of sound reduction properties to help preserve sleep and to protect privacy and accuracy of communication in support of HIPAA compliance and medical error reduction.
According to the Veterans Administration’s “Design Guide for Inpatient Mental Health & Residential Rehabilitation Treatment Program Facilities”:32
A mental health facility requires special attention to sound control. Acoustic isolation shall be provided from the units to other areas in the hospital and inside each patient and resident room to preserve privacy/confidentiality and to reduce excessive noise. Excessive noise can negatively impact a therapeutic environment for the patient/resident and the staff. It may affect one’s ability to hear or be heard in a normal speaking tone, which detracts from a calm, nonthreatening environment. Excessive noise may heighten some patients’ fear and anxiety levels.
Impact Resistance and Durability
Patients in behavioral and mental health settings may become violent. Such incidents potentially cause more impact on flooring in these spaces than in traditional healthcare settings. This calls for the highest level of impact-resistant and durable flooring.
Durability Considerations for Spaces in Continual Use
Flooring that does not need to be stripped, waxed, and recoated is most beneficial for a BMH center. The noise associated with maintenance protocol could negatively impact the serene ambiance at the heart of healing. Even more disruptions occur if the flooring needs replacing. A no-finish floor and durable flooring sustain the rigor of the setting, reduce the associated person-hours to maintain, and mitigate noise.
CONCLUSION
A debt of gratitude is owed to architects, designers, and care centers for normalizing the patient experience in behavioral and mental healthcare settings.
The VA Design Guide Mental Health Facilities Design Guide identifies key criteria in the selection of interior finishes, and those also apply to flooring selection, such as aesthetic value, therapeutic attributes, maintainability, durability, infection control sustainability, and safety and security.
The Advisory Board notes that inequities in behavioral healthcare impact the financial outcomes of healthcare organizations. Despite high and growing demand, access to reliable behavioral health services is challenging. Provider shortages, stigma, and limited reimbursement create significant barriers to timely, cost-effective behavioral healthcare.
They go on to share that improving behavioral health has the potential to significantly improve clinical outcomes and healthcare costs. Behavioral health conditions are prevalent. Approximately 70 percent of patients with a behavioral health condition have a medical comorbidity. Additionally, “deaths of despair” (from alcohol, drugs, or suicide) have more than doubled since 1999. Despite the prevalence of behavioral health conditions, they often go untreated. Less than half of patients receive treatment.
By many accounts, behavioral and mental healthcare and acuity levels continue to increase. Mental health experts interviewed by Forbes33 listed some areas of increase: social media-induced anxiety, work burnout, eating disorders, and neurodivergent conditions affecting mental health. For NAMI, the National Alliance on Mental Illness, three future goals34 stand out: 1) To help people get help sooner, 2) to help them get the best care possible, and 3) to detach mental healthcare needs from law enforcement. All signs point to an overarching need for more spaces for those with mental and behavioral health challenges and those who care for them. This is why the floor matters: as a foundation for therapeutic care that allows patients to heal and transition back to whole, healthy lives in a society that supports their healing.
ENDNOTES
1“Behavioral Health: Cheat Sheet.” Advisory Board. 6 May 2020. Web. 27 September 2023.
2“Treatment Settings.” National Alliance on Mental Health. Web. 27 September 2023.
3Card, A., Taylor, E., Piatkowski, M. “Design for Behavioral and Mental Health: More Than Just Safety.” The Center for Health Design. 2018. Web. 27 Sept. 2023.
4“Behavioral & Mental Health.” The Center for Health Design. Web. 27 September 2023.
5Card, A., Taylor, E., Piatkowski, M. “Design for Behavioral and Mental Health: More Than Just Safety.” The Center for Health Design. 2018. Web. 27 Sept. 2023.
6“About Us.” The Center for Health Design. Web. 27 September 2023.
7,8“Safety Risk Assessment Tool.“ The Center for Health Design. 2014, 2017. Web. 27 September 2023.
9,10McMurray, K.N. “Behavioral Health Design Guide.” January 2022. Web. 27 September 2023.
11Abushusheh, Addie, Taylor, Ellen. “Memory Care: The Intersection of Aging and Mental Health.” The Center for Health Design. January 2020. Web. 27 September 2023.
12Browning, William; Ryan, Catherine; Clancy, Joseph. “14 Patterns of Biophilic Design.” Terrapin Bright Green. 2014. Web. 27 September 2023.
13Grinde B, Patil GG. “Biophilia: does visual contact with nature impact on health and well-being?” International Journal of Environmental Research and Public Health. 6 September 2009. Web. 27 September 2023.
14Browning, William, Ryan, Catherine, Clancy, Joseph. “14 Patterns of Biophilic Design.” Terrapin Bright Green. 2014. Web. 27 September 2023.
15Piche, Mary-Ellen, Luna, Gina. “Designing an Evidence-Based Healing Environment.” American College of Healthcare Executives. Web. 27 September 2023.
16Johnson J., Hall L.H., Berzins K., Baker J., Melling K., Thompson C. “Mental healthcare staff well-being and burnout: A narrative review of trends, causes, implications, and recommendations for future interventions. International Journal of Mental Health Nursing. 2018. Web. 27 September 2023.
17Shanafelt T.D., Balch C.M., Bechamps G.J., Russell T., Dyrbye L., Satele D., Collicott P., Novotny P.J., Sloan J., Freischlag J.A. “Burnout and career satisfaction among American surgeons.” Annals of Surgery. 2009 Web. 27 September 2023.
18Nanda, U., Malone, E., and Joseph, A. ). Achieving EBD Goals through Flooring Selection & Design.” 2012. The Center for Health Design. Web. 27 September 2023.
19Florence CS, Bergen G, Atherly A, Burns ER, Stevens JA, Drake C. “Medical Costs of Fatal and Nonfatal Falls in Older Adults.” Journal of the American Geriatrics Society. March 2018. Web. 27 September 2023.
20“Promoting Patient Safety.” Patient Safety Network. Web. 27 September 2023.
21Ulrich, R. S., Zimring, C., Zhu, X., DuBose, J., Seo, H. B., Choi, Y. S., ... & Joseph, A. 2008. “A review of the research literature on evidence-based healthcare design.” HERD: Health Environments Research & Design Journal. 2008. Web. 27 September 2023.
22Bae, S., & Fabry, D. (2014). “Assessing the relationships between nurse work hours/overtime and nurse and patient outcomes: Systematic literature review.” Nursing Outlook. March-April 2014. Web. 27 September 2023. < https://pubmed.ncbi.nlm.nih.gov/24345613/>
23Trinkoff, A. M., Johantgen, M., Storr, C. L., Gurses, A. P., Liang, Y., & Han, K. “Nurses’ work schedule characteristics, nurse staffing, and patient mortality.” Nursing Research. January-February 2011. Web. 27 September 2023.
24,25“Design Guide for Inpatient Mental Health & Residential Rehabilitation Treatment Program Facilities.” U.S. Department of Veterans Affairs. January 2021. Web. 27 September 2023.
26“Healthy Flooring.” Healthcare Without Harm.” Web. 27 Sept. 2023.
27“Design Guide for Inpatient Mental Health & Residential Rehabilitation Treatment Program Facilities.” U.S. Department of Veterans Affairs. January 2021. Web. 27 September 2023.
28Harris, D. D., & Detke, L. A. (2013). The role of flooring as a design element affecting patient and healthcare worker safety. HERD: Health Environments Research & Design Journal, 6(3), 95-119.
29Moussatche, H., & Languel, J. (2002). Life cycle costing of interior materials for Florida’s schools. Journal of Interior Design, 28(2), 37-49.
30,31,32“Design Guide for Inpatient Mental Health & Residential Rehabilitation Treatment Program Facilities.” U.S. Department of Veterans Affairs. January 2021. Web. 27 September 2023. <
33Butkovic, Marija. “6 Experts Weight In On The Present And The Future Of Mental Health.” Forbes. 11 July 2022. Web. 27 September 2023.
34“A Bridge Between Our Rich History and Future Opportunities.” National Alliance on Mental Illness. Web. 27 September 2023. https://nami.org/NAMInet/Board-of-Directors/Governance-Documents/NAMIStrategicPlan2020
Sandra Soraci EDAC, LEED AP, NCIDQ, is the Director of Healthcare and Senior Living Segment Strategy, for Tarkett NA. Sandra’s diverse and deep career-specific focus on healthcare and commercialization efforts fully informs the customer decision-making journey. Flooring is no longer a design feature, it is an investment in health and safety, and we all have a stake in improving outcomes for our customers. Healthy environments support the healing process, and that begins at the ground level, with the floor. Through an evidence-based design lens, Tarkett Flooring continually seeks to create flooring solutions that contribute to greater connection, safety, and overall well-being. Healthcare is ever-changing; my passion is to educate, elevate, and transform sales enablement to fully support what our healthcare customers tell us they need the floor to do.
Kathy Price-Robinson is a nationally known writer focusing on building and architecture. Her award-winning remodeling series ran 13 years in the Los Angeles Times. She has written for dozens of publications in the design and building industry and developed more than 100 continuing education.
A 2023 study by Mental Health America identified that 5.44 percent of adults experience severe mental illness. More than 12.1 million adults (4.8 percent) have reported serious thoughts of suicide. This is why “place” matters.

Photo courtesy of Ben Rahn/A-Frame
To enhance healing, settings for behavioral and mental healthcare need to balance safety with a warm, comfortable atmosphere. That includes plants, views of nature, natural wood, places to socialize, resilient flooring, and soft colors. Project: Michael Garron Hospital, inpatient mental health units designed by B+H Architects, Toronto, Canada.
The Advisory Board, which focuses on healthcare research,1 states, “Behavioral health encompasses people’s psychological well-being and ability to function in everyday life. Behavioral health conditions include mental illness disorders and substance abuse disorders.” They also note, “Health systems are increasingly recognizing that behavioral health is an essential part of physical and population health.” There is a growing demand for centers to support behavioral and mental health issues, yet access to reliable behavioral health services is challenging. When the opportunity to design new construction or renovation presents itself, this educational unit will provide oversight and baseline considerations. There is an overarching need for centers to provide effective, specialized residential, inpatient, and outpatient treatment. Demand facilitates that architects and designers will be tasked with planning and constructing care centers in various geographic settings. While these facilities fall into the healthcare category, aesthetically and functionally they require a different design approach. Evidence-based research shows that behavioral and mental health patients heal better in a warm and welcoming environment. There is concern patients may self-harm or harm others, which requires a unique level of detail for safety with interior finishes. There is a defining need for a calming, homelike aesthetic balance. The floor is the foundation; it supports all activities and can have an actionable impact on fostering safety and outcomes. This educational course demonstrates the design guidelines and needs of behavioral and mental healthcare center facilities. The Advisory Board shares that “Treating patients with behavioral health diagnoses costs about $900 more per month than patients without such diagnoses.” This is why the floor matters, from the subfloor to the surface finish, to have an actionable impact on outcomes.
THE NEED FOR EVIDENCE-BASED DESIGN FOR BEHAVIORAL AND MENTAL HEALTHCARE ENVIRONMENTS
The Advisory Board states that regardless of demographic group, patients with behavioral health conditions experience unique inequities compared to patients with only physical health conditions. The pandemic and its ripple effects only exacerbated an existing crisis in the U.S. The behavioral healthcare sector struggles with a unique "meta" inequity. So, when given the opportunity to design a BMH center, apply evidence-based design principles.
According to the National Institute of Mental Health, the spectrum of behavioral and mental health (BMH) conditions includes anxiety, attention deficit disorders, autism spectrum disorders, bipolar disorders, depression, obsessive-compulsive disorders, post-traumatic stress disorder (PTSD), substance abuse, and suicide, among others.3
Behavioral health treatment has undergone a shift, as have the means of delivery, which enables new centers that support a normalizing environment to ensure a return to a productive life within the community. Treating people who have mental illness is critically important. However, how and where to do so is not always clear. Some emergency rooms are not well equipped with crisis intervention spaces to treat patients of varying acuity levels. Increasingly, centers specifically created to treat individuals experiencing behavioral and mental health crises are desperately needed.

Photo courtesy of Ben Rahn/A-Frame
In behavior and mental healthcare facilities, biophilic features, warm colors, and the right flooring specification for the right place benefit not only patients but also staff, care providers, and visitors. Project: Michael Garron Hospital, inpatient mental health units designed by B+H Architects, Toronto, Canada.
Behavioral and Mental Healthcare is Cost-Effective
Understanding that behavioral and mental health conditions affect one in five adults in the U.S. each year, these illnesses are even more common among patients receiving care for medical conditions. According to The Center for Health Design (CHD)4, which provides guidance for the safe and therapeutic design of healthcare facilities, “Up to 45% of patients admitted to the hospital for a medical condition or presenting to the emergency department with a minor injury also have a concurrent BMH condition.” The Center states these comorbidities “increase the risk of psychological harm associated with care.” Therefore, providing BMH patients with a healing, therapeutic environment is an overarching design driver in these care settings. “Design interventions aimed at improving the psychological well-being of patients with BMH comorbidities may be more cost-effective than they initially appear, because they can be leveraged to support improved well-being for other populations as well, including other patients, staff, and visitors,” according to the CHD.
Design for facilities to care for this patient type is complex. Types of mental health facilities include:
- Crisis Units
- Residential mental health facilities
- Psychiatric hospitals (inpatient)
- Hospital environment
- Behavioral health clinics
- Pediatric and adolescent adult
- Memory enhancement centers for dementia
- Mental health rehabilitation (outpatient rehab – intensive or traditional)
McLean Hospital, a member of Mass General Brigham in Massachusetts, the largest psychiatric affiliate of Harvard Medical School, is America’s number one hospital for psychiatric care, according to the latest U.S. News & World Report annual “Best Hospitals” survey. While the facility treats serious psychiatric conditions based on the latest research, they recognize that a homelike setting is the best place to heal physically, mentally, and emotionally. Here is how they describe their residential treatment facility: “The Pavilion, located on McLean’s historic main campus, offers patients a peaceful treatment setting. Our comfortable environment, attractive decor, and range of high-quality amenities are designed to help individuals focus on treatment as well as their overall health and well-being.”
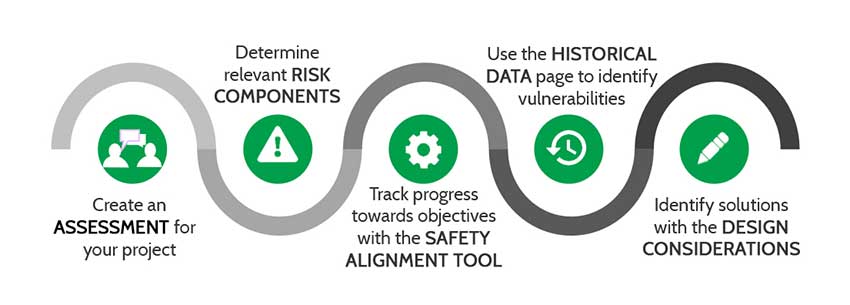
Photo courtesy of The Center for Health Design
A Safety Risk Assessment can be approached systematically.
Human-Centered Design
There is compelling evidence5 that certain design features support healing and psychological well-being in BMH settings. The CHD offers this list:
- A homelike, deinstitutionalized environment that supports patient autonomy and control over their own environment
- A well-maintained and well-organized environment
- Noise control
- Support for privacy
- Access to daylight and views of nature
- Physical access to the outdoors
- Support for feelings of personal safety/security
- Support for social interaction
- Positive distraction
PRIMARY RESOURCES RELATED TO BEHAVIORAL AND MENTAL HEALTH FACILITIES FOR THE DESIGN COMMUNITY
Credible research informs design decisions of the physical environment to encourage the experience of care and allow clinical staff and patients to heal together. These resources support appropriate design decisions:
The Center for Health Design: Evidence-Based Design (EBD)
The Center for Health Design (CHD)6 launched in 1993 as a team of forward thinkers with a vision for creating healthcare facilities that promote healthier environments for patients and staff. CHD is widely credited with defining EBD as “the deliberate attempt to base building decisions on the best available research evidence with the goal of improving outcomes and of continuing to monitor the success or failure for subsequent decision-making.” The CHD is a leading knowledge repository force in transforming hospitals, clinics, wellness centers, doctor’s offices, and residential care facilities through design research, education, and advocacy.
The Knowledge Repository
CHD also offers access to the knowledge repository, a complete, user-friendly database of references to healthcare design research that continues to grow with the latest peer-reviewed publications.
Safety Risk Assessment Tool
The CHD developed the Safety Risk Assessment (SRA). The Facilities Guideline Institute (FGI) Guidelines Section 1.2-4 requires a Safety Risk Assessment (SRA)7 to determine the level of risk acceptable for both patients and staff in each part of the patient-accessible areas of behavioral health units. The SRA Report is vital and must be consulted in reaching all safety-related design decisions.
What is the SRA?
The Safety Risk Assessment (SRA) Toolkit is:
- A proactive process that can mitigate risk
- A discussion prompt for a multidisciplinary team
- An evidence-based design (EBD) approach to identify solutions.
The SRA targets six areas of safety (infections, falls, medication errors, security, injuries of behavioral health, and patient handling) as required in the FGI Guidelines.
A Systematic Approach for Creating a Safety Risk Assessment8
From this collaborative effort, informed selection, specification, and procurement for BMH centers, including the flooring, will be gleaned.
Behavioral Health Design Guide
The Behavioral Health Design Guide9 is updated frequently to keep pace with new knowledge about patient safety and new products for use in behavioral health facilities.
The Guide addresses patient safety in the built environment for the adult inpatient mental and behavioral healthcare units according to how the space is used by patients and rates those spaces I through V (see next page). Level I areas are those that patients cannot access and, therefore, pose the least concern. Level V areas are those where patients and staff interact and where patient behavior is unpredictable, thus posing the most significant concern. The Guide’s authors describe each area’s obvious and latent hazards and offer insights into reducing risks with thoughtful design and appropriate furniture and fixtures.
VA Design Guide for Inpatient Mental Health & Residential Rehabilitation Treatment Program Facilities
This Veterans Administration Guide for Inpatient Mental Health & Residential Rehabilitation Treatment Program Facilities sets the standards for treating veterans. It is also a useful guide for non-veteran facilities. As with other guides, this one seeks to balance a welcoming, nurturing environment with a safe setting for patients, staff, caregivers, and visitors.
Secure installation specific to the floor and wall base prevents flooring from being torn or removed by inpatients to cause harm to themselves or others. Floors with high glare may adversely impact visual perception for psychotic and older patients and, therefore, should be avoided. Suitable flooring considerations include resilient sheet, linoleum, and sheet vinyl flooring. Seclusion Rooms require flooring with an integral base and floor-to-ceiling and wall-to-wall resilient wall protection or rigid wall panels.
To achieve a more homelike environment, resilient sheet, rubber, linoleum, and sheet vinyl flooring with wood grain appearance may be used in some areas or throughout the unit. Accent or other patterns are also available and may help with wayfinding. A flooring that does not require floor finish is highly recommended.
Due to its homelike feel, sound absorption, and ease of replacement, carpet tile is recommended as a flooring option in certain areas. Carpet tile should have an upgraded moisture guard or moisture-resistant backing system. Carpet tile should be used only in supervised patient areas such as group therapy, day rooms, dining rooms, intake/interview rooms, recreation/activity areas, and staff areas such as conference rooms and office areas. Hybrid resilient sheet flooring solutions provide the look, feel, and noise control and moisture qualities of carpet while also creating a surface to address infection control, cleaning, and ease of maintenance.
Facilities Guidelines Institute (FGI)
The Guidelines for Design and Construction documents are updated every four years to keep pace with evolving care delivery models, facility types, and requests for up-to-date guidance from care providers, designers, and regulators.
For the 2022 edition, the Facility Guidelines Institute (FGI) has published three Guidelines for Design and Construction standards with distinct planning and design requirements for hospitals (including behavioral and mental health), outpatient facilities and residential health facilities, residential care and support facilities, and nonresidential support facilities.
The Guideline’s standards are important in planning, design, and construction because federal agencies, states, and local jurisdictions adopt them as law and apply them as a standard against which to evaluate building projects. Though they are guidelines and not building codes at a federal or state level, they hold tremendous weight in the design and decision-making process as a path to compliance and minimum requirements.
FGI Guidelines Impact Flooring Selection, Specification, and Procurement
Flooring can have an actionable impact on operational optimization and clinical efficiency, reduce associated person-hours to maintain, and reduce the total cost of ownership. These product attributes result in optimized processes and effective life cycle costs over time—all sustainably. Flooring can positively impact patient experience, mitigate cross-contamination, foster safety, and reduce caregiver fatigue. Flooring should be viewed as a system, from the subfloor to the surface finish. In support of specifying the right product for the right space, the FGI Guidelines are a source to ensure the right flooring product is specified in support of health, wellness, and safety.
Flooring specification in the BMH setting; safety is paramount to prevent patients from potentially harming themselves or their caregivers. Flooring installation detail in high-risk areas must mitigate weaponization and self-harm.
FGI, Behavioral Health Design Guide, and the New York State Design Guide speak to these four categories for flooring details:
- No flooring cap
- Tamper-resistant
- Impact-resistant
- Water-resistant/cleanable
The proper design of facilities for BMH patients is both highly consequential and complex. If not specialized in the BMH setting, architects and designers often collaborate with highly experienced consultants in the specialized field.
THE IMPACT OF INTERIOR FINISHES ON PATIENTS’, RESIDENTS’, STAFF, AND CAREGIVERS’ COGNITIVE, EMOTIONAL, PSYCHOSOCIAL, AND PHYSICAL NEEDS
In an issue brief, CHD notes that most design teams acknowledge that providing BMH patients with a healing, therapeutic environment should be an important goal for health design. However, the evidence base for designing for BMH in medically oriented healthcare facilities has focused almost exclusively on physical safety. While safety is obviously the right place for the healthcare design community to start when designing for BMH, it is clearly not the right place to stop.
Finishes and furnishings in behavioral and mental health centers can be subjected to abuse. Materiality matters to withstand daily demands and heavy use. Carefully consider the selection, specification, and procurement of interior finishes, including the flooring, as it can impact the cognitive, emotional, psychosocial, and physical needs of patients, residents, staff, and caregivers.
In selecting and specifying interior finishes, specialty manufacturers focus on safety features while mitigating an institutional look and feel. Supporting the needs of safety and healing enables the transition of care from inpatient to outpatient or residential care with a homelike setting.
The Intersection of Aging, Behavioral, and Mental Health
In a brief on the connection between aging and mental health,11 the Center for Health Design notes that by 2031, the largest segment of the U.S. population—the Baby Boom generation—will reach the age of 85. At this age, the brief notes, people experience the most significant and extreme effects of the normal changes associated with aging. It is also the age associated with the highest risk of developing dementia, particularly Alzheimer’s disease.
Many design features that serve BMH patients also serve those in memory enhancement facilities, including a homelike setting and access to nature and natural environments. Further benefits include simplifying the layout of the spaces, reducing the scale, enabling interactions between those with and without dementia, and personalizing bedrooms.
As the need increases for both BMH and dementia care, research and experience concerning therapeutic and safe design can serve both interests.

Photo courtesy of Tarkett
The flooring pattern can evoke scenes from nature and calm patients with soft, soothing colors.
Human Connection to the Natural World
Metropolis magazine shared that if the design doesn’t focus on aspects of the natural world that contribute to human health and productivity in the age-old struggle to be fit and survive, it’s not biophilic. Simply put, biophilic design focuses on those aspects of the natural world that have contributed to human health and productivity. Another distinguishing feature of biophilic design is its emphasis on the overall setting or habitat and not a single or isolated occurrence of nature.
The magazine shares that biophilic design depends on repeated and sustained engagement with nature. An occasional, transient, or isolated experience of nature exerts only superficial and fleeting effects on people and can sometimes be at variance with fostering beneficial outcomes. Biophilic design requires reinforcing and integrating design interventions that connect with the overall setting or space.
Biophilic design fosters positive and sustained interactions and relationships among people and the natural environment. Humans are a profoundly social species whose security and productivity depend on positive interactions within a spatial context. Effective biophilic design fosters connections between people and their environment, enhancing feelings of relationship and a sense of membership in a meaningful community.
According to the respected Terrapin Bright Green consulting group: ‘Biophilic design can reduce stress, enhance creativity and clarity of thought, improve our well-being and expedite healing; as the world population continues to urbanize, these qualities are ever more important. Theorists, research scientists, and design practitioners have been working for decades to define aspects of nature that most impact our satisfaction with the built environment.”12
Conversely, the absence of these principles in the built environment can impact human health. According to a paper in the International Journal of Environmental Research and Public Health, “It is concluded that an environment devoid of Nature may act as a ‘discord,’ i.e., have a negative effect.”13
Terrapin Bright Green offers 14 Patterns of Biophilic Design14 that articulate the relationships between nature, human biology, and the design of the built environment so that building occupants can experience the human benefits of biophilia in design applications.
They are:
Nature in the Space Patterns
- Visual connection with nature
- Non-visual connection with nature
- Non-rhythmic sensory stimuli
- Thermal and airflow variability
- Presence of water
- Dynamic and diffuse light
- Connection with natural systems
Natural Analogues Patterns
- Biomorphic forms and patterns
- Material connections with nature
- Complexity and order
Nature of the Space Patterns
- Prospect
- Refuge
- Mystery
- Risk/peril
Creating Healing Environments
Person-centered design in the healthcare setting has undergone a paradigm shift to incorporate more efficient healing designs. Much evidence in the literature supports the innovations now being used to design the built environment to optimize healing and to foster the healing environment for behavioral and mental healthcare, for the patient, resident, caregiver, staff, and family, specific to the floor.15
Soothing colors—For creating an environment that is calming rather than exciting, soothing, muted colors.
Colors and patterns that reflect local geography—These features could help make the patients feel more at home.
Respite areas—According to the National Institutes of Health, “Healthcare workers are particularly susceptible to burnout.16
Burnout among healthcare workers can adversely affect their performance with a ripple effect across the healthcare system. It increases the risk of medical errors and adversely affects patients’ safety.”17 A therapeutic environment geared toward patients would also benefit the staff and healthcare workers and increase employee retention. Respite areas support the caregiver to alleviate workplace stressors, even for only fifteen minutes. Bringing wood tones with flooring can support the connection to nature.
WHY THE FLOOR MATTERS—FROM THE SUBFLOOR TO THE SURFACE FINISH
Flooring is integral to achieving the safety and aesthetics that best serve the behavioral healthcare facility patients, residents, staff, caregivers, and visitors. The flooring system, from the subfloor to the aesthetic surface finish, sets the stage for all healthcare activities, and its selection and specification can impact multiple health-related outcomes.
Think of the flooring manufacturer as another layer to risk management to mitigate critical impacts, increase safety, maximize efficiency, and capture ROI. The finished floor is only as good as the integrity of the subfloor and the maintenance program established to maintain the flooring. As a solutions expert, the manufacturer is your partner, focusing on flooring as an integrated project team member.
A flooring project has five main phases, each vital to a successful installation meeting customer expectations.
- Product selection/specification
- Pre-installation
- Installation
- Post-Installation
- Maintenance
Flooring and the Eight Goals of Evidence-Based Design
To begin the discussion of the floor, consider the Eight Goals of Evidence-Based Design and how flooring helps achieve them. Based on research from The Center for Health Design, these eight goals inform and support how performance characteristics of flooring materials can have an actionable impact on the health system’s effectiveness and revenue.18

Photo courtesy of Tarkett
The flooring is the foundation for the entire healing atmosphere.
EBD Goal 1: Reduce slips, trips, and falls
- Medical spending for fatal falls was estimated to be $754 million annually.19
- Avoid complex patterns, color stimulation, and reflective surfaces.
- Ensure transitions between surfaces are seamless and color-matched to mitigate certain patients from becoming fixated on the material and picking at it.
2. EBD Goal 2: Reduce patient and staff injuries associated with falls
- The Centers for Medicare and Medicaid Services (CMS) no longer pay for any additional costs associated with “never events.” Falls with injury are a serious reportable “never-event” and are non-reimbursable to the health system.20
- Utilize varying light reflectance values (LRV) as a means of identifying differences in height between areas.
3. EBD Goal 3: Reduce noise levels
- In healthcare environments, evidence suggests that increased noise levels can have a measurable impact on both the patient and staff experience.21
- Material selection that can mitigate in-room impact sound.
4. EBD Goal 4: Reduce staff fatigue
- Nurse fatigue can profoundly impact adverse patient outcomes, such as patient mortality and medication errors, as well as individual adverse nurse outcomes, including musculoskeletal injuries, emotional disorders, and job burnout. Finishes can support staff physically and cognitively.22,23
- Artwork can reduce environmental stressors and patient aggression.24
5. EBD Goal 5: Reduce surface contamination and potential risk of healthcare-associated Infections (HAI)
- Products within the healing environment must support human health. The Advisory Board, a leading healthcare research group, stated, “Suppliers who produce materials that passively fight infection without added antimicrobials have a high value.” In 2003, the CDC noted that no evidence was available to suggest that using products treated with antimicrobial chemicals would make patients healthier or prevent disease.
- Flooring materials need to withstand heavy use and abuse and be easily repairable. Consider product composition, construction, and installation details.25
- Monolithic sheet vinyl with integral base and heat welded seams.
6. EBD Goal 6: Improve indoor air quality (IAQ)
- Every day, patients and healthcare workers are exposed to an array of chemicals. Many of these chemicals have been shown to impact individual health and the environment negatively.26
- Flooring materials and maintenance protocols need to foster positive indoor air quality.27
- Specify certified asthma and allergy-friendly flooring solutions.
7. EBD Goal 7: Improve patient and family satisfaction
- Flooring can substantially contribute to patient experience, safety, and outcomes and is a critical capital investment decision for healthcare facilities.28
- Avoid distracting patterns, color combinations, and large chips to mitigate visual misperceptions, particularly among those with schizophrenia and dementia.
8. EBD Goal 8: Represent the best return on investment
- When making design decisions, it is crucial to evaluate a flooring material’s long-term cost-effectiveness in relation to its initial costs.29
- Durability is key as weighted furniture is dragged, and the floor can scuff, scratch, or gouge.
- Monolithic floor installation mitigates pick points that are always a concern. Downtime for replacement flooring in this setting can have financial implications if a unit or space needs to be shut down.30

Photo courtesy of Tarkett
Homogeneous floors benefit patients, staff, caregivers, and visitors.
Safety Factors to Consider when Specifying and Installing Flooring for Behavioral and Mental Healthcare Centers
Consider these factors when specifying flooring for these specialized facilities:
Benefits of Homogeneous Floors in BMH Facilities
- Homogenous sheet vinyl heat welded to create a virtually seamless, water-tight, monolithic surface, eliminating potential pick and ligature points.
- No floor finish ever.
- Durable–can withstand high static and traffic loads.
- Can be used in hallways, common spaces, patient rooms, labs, back of house.
- Supports infection control protocol.
- Holds up to medical staining agents, scratches, and chemicals.
- Ideal for Level 3 and Level 4 patient care areas: seclusion rooms, admission rooms, and quiet rooms.
Slip-resistant vinyl flooring: A flooring solution for heavy-traffic wet areas where safety is of utmost importance. It provides a confident grip for bare feet and reduces the risk of slipping. Suitable for corridors and back-of-house areas.
Hybrid resilient sheet flooring: A heterogeneous construction of nylon and closed-cell cushion fused through heat and pressure, making the layers integral and inseparable. The innovative closed-cell cushion is the most significant component of performance and design capabilities. Seamless flooring is much harder for patients to pick at and potentially hurt themselves. Suitable for corridors, common spaces, therapy areas, and dining areas.
Installation Detail for Pick Resistance
The product and installation should resist picking, preventing parts of the flooring system from being picked off and becoming a tool for harm. Covings should be tightly adhered to the wall.
Ease of Wayfinding and Circulation Cues
Wayfinding helps patients and visitors navigate a facility with minimal assistance and no confusion. Flooring color can identify room types and patterns to guide people toward their destination.
According to the VA design guide for behavioral and mental health facilities, “Design can support elements by using color to identify program areas. For example, a consistent color can identify all staff off-stage areas. Patient units can be identified by distinct and different color palettes. Group Rooms may be identified with consistent color.”31
FGI Guidelines speak to pattern and color contrast research. Patterns and contrast research suggest that flooring with a medium-sized pattern (1 to 6 inches wide, or 2.54 to 15.24 centimeters wide) was associated with more falls than floors with no design or a small pattern (less than 1 inch wide, or 2.54 centimeters wide), or a large pattern (wider than 6 inches). High-contrast patterns with large geometric or swirling designs on floor surfaces have been associated with more patient falls. These patterns can distract and potentially confuse persons with visual acuity issues.
Minimal Contrast Between Types of Flooring
In the United States, 8 percent of the population (26.M), and 1:5 who are over sixty-five are visually impaired. Similar values between different flooring materials help minimize transitions between different types of flooring and may reduce fall risk. Smooth transitions should be provided between different flooring materials. Flush thresholds should be used to reduce tripping hazards. Some flooring types, such as resilient flooring (e.g., rubber, luxury vinyl tile, sheet vinyl) and carpet, should include transition strips that minimize trip hazards.
Slip Resistance
The slip-resistance ratings of flooring surfaces should be appropriate for the area of use—for dry or wet conditions and use on ramps and slopes.
According to FGI 2022 Guidelines for Design & Construction of Hospitals: Wet conditions are common in areas such as kitchens and bathing areas, entries from exterior to interior space, and areas where water is used for patient services. Slip resistance is also an important consideration for ramps and stairways. In dry areas, soft flooring (e.g., carpet, cushioned flooring) can reduce the risk of falls and the impact of associated injuries.
Compatible with Wheeled Devices
Floor surfaces should allow easy movement of all wheeled equipment in the facility. Portable lifting equipment without powered wheels may require more exertion by staff than ceiling-mounted equipment to move an elevated patient around and through a space. The exertion required by staff may increase with the use of carpet; however, different types and brands of carpet may have significantly different levels of resistance to wheeled devices. Installation of a mock-up to test hybrid flooring materials with wheeled equipment and devices used in a facility is recommended. Carpet should not be automatically discounted as inappropriate due to this challenge, as it has significant advantages over hard-surface flooring in terms of noise reduction and acoustics.
Floor Reflectivity and Glare
Finished floors with a high gloss value cause glare that may compromise patient vision by being misinterpreted as a pool of water on the floor or a hole in the floor surface, disrupting the balance. The use of no floor finish flooring eliminates glare. Where a floor finish is required, smooth flooring surfaces should be sealed with a matte finish to reduce surface glare. A minimum LRV of 30 is recommended between floors and walls (wall bases should match the walls) to help define the space.
Sound Attenuation (Reduce Impact Sound)
Reducing impact sound requires specifying the right product for the right space. Acoustic floors should be selected with consideration of sound reduction properties to help preserve sleep and to protect privacy and accuracy of communication in support of HIPAA compliance and medical error reduction.
According to the Veterans Administration’s “Design Guide for Inpatient Mental Health & Residential Rehabilitation Treatment Program Facilities”:32
A mental health facility requires special attention to sound control. Acoustic isolation shall be provided from the units to other areas in the hospital and inside each patient and resident room to preserve privacy/confidentiality and to reduce excessive noise. Excessive noise can negatively impact a therapeutic environment for the patient/resident and the staff. It may affect one’s ability to hear or be heard in a normal speaking tone, which detracts from a calm, nonthreatening environment. Excessive noise may heighten some patients’ fear and anxiety levels.
Impact Resistance and Durability
Patients in behavioral and mental health settings may become violent. Such incidents potentially cause more impact on flooring in these spaces than in traditional healthcare settings. This calls for the highest level of impact-resistant and durable flooring.
Durability Considerations for Spaces in Continual Use
Flooring that does not need to be stripped, waxed, and recoated is most beneficial for a BMH center. The noise associated with maintenance protocol could negatively impact the serene ambiance at the heart of healing. Even more disruptions occur if the flooring needs replacing. A no-finish floor and durable flooring sustain the rigor of the setting, reduce the associated person-hours to maintain, and mitigate noise.
CONCLUSION
A debt of gratitude is owed to architects, designers, and care centers for normalizing the patient experience in behavioral and mental healthcare settings.
The VA Design Guide Mental Health Facilities Design Guide identifies key criteria in the selection of interior finishes, and those also apply to flooring selection, such as aesthetic value, therapeutic attributes, maintainability, durability, infection control sustainability, and safety and security.
The Advisory Board notes that inequities in behavioral healthcare impact the financial outcomes of healthcare organizations. Despite high and growing demand, access to reliable behavioral health services is challenging. Provider shortages, stigma, and limited reimbursement create significant barriers to timely, cost-effective behavioral healthcare.
They go on to share that improving behavioral health has the potential to significantly improve clinical outcomes and healthcare costs. Behavioral health conditions are prevalent. Approximately 70 percent of patients with a behavioral health condition have a medical comorbidity. Additionally, “deaths of despair” (from alcohol, drugs, or suicide) have more than doubled since 1999. Despite the prevalence of behavioral health conditions, they often go untreated. Less than half of patients receive treatment.
By many accounts, behavioral and mental healthcare and acuity levels continue to increase. Mental health experts interviewed by Forbes33 listed some areas of increase: social media-induced anxiety, work burnout, eating disorders, and neurodivergent conditions affecting mental health. For NAMI, the National Alliance on Mental Illness, three future goals34 stand out: 1) To help people get help sooner, 2) to help them get the best care possible, and 3) to detach mental healthcare needs from law enforcement. All signs point to an overarching need for more spaces for those with mental and behavioral health challenges and those who care for them. This is why the floor matters: as a foundation for therapeutic care that allows patients to heal and transition back to whole, healthy lives in a society that supports their healing.
ENDNOTES
1“Behavioral Health: Cheat Sheet.” Advisory Board. 6 May 2020. Web. 27 September 2023.
2“Treatment Settings.” National Alliance on Mental Health. Web. 27 September 2023.
3Card, A., Taylor, E., Piatkowski, M. “Design for Behavioral and Mental Health: More Than Just Safety.” The Center for Health Design. 2018. Web. 27 Sept. 2023.
4“Behavioral & Mental Health.” The Center for Health Design. Web. 27 September 2023.
5Card, A., Taylor, E., Piatkowski, M. “Design for Behavioral and Mental Health: More Than Just Safety.” The Center for Health Design. 2018. Web. 27 Sept. 2023.
6“About Us.” The Center for Health Design. Web. 27 September 2023.
7,8“Safety Risk Assessment Tool.“ The Center for Health Design. 2014, 2017. Web. 27 September 2023.
9,10McMurray, K.N. “Behavioral Health Design Guide.” January 2022. Web. 27 September 2023.
11Abushusheh, Addie, Taylor, Ellen. “Memory Care: The Intersection of Aging and Mental Health.” The Center for Health Design. January 2020. Web. 27 September 2023.
12Browning, William; Ryan, Catherine; Clancy, Joseph. “14 Patterns of Biophilic Design.” Terrapin Bright Green. 2014. Web. 27 September 2023.
13Grinde B, Patil GG. “Biophilia: does visual contact with nature impact on health and well-being?” International Journal of Environmental Research and Public Health. 6 September 2009. Web. 27 September 2023.
14Browning, William, Ryan, Catherine, Clancy, Joseph. “14 Patterns of Biophilic Design.” Terrapin Bright Green. 2014. Web. 27 September 2023.
15Piche, Mary-Ellen, Luna, Gina. “Designing an Evidence-Based Healing Environment.” American College of Healthcare Executives. Web. 27 September 2023.
16Johnson J., Hall L.H., Berzins K., Baker J., Melling K., Thompson C. “Mental healthcare staff well-being and burnout: A narrative review of trends, causes, implications, and recommendations for future interventions. International Journal of Mental Health Nursing. 2018. Web. 27 September 2023.
17Shanafelt T.D., Balch C.M., Bechamps G.J., Russell T., Dyrbye L., Satele D., Collicott P., Novotny P.J., Sloan J., Freischlag J.A. “Burnout and career satisfaction among American surgeons.” Annals of Surgery. 2009 Web. 27 September 2023.
18Nanda, U., Malone, E., and Joseph, A. ). Achieving EBD Goals through Flooring Selection & Design.” 2012. The Center for Health Design. Web. 27 September 2023.
19Florence CS, Bergen G, Atherly A, Burns ER, Stevens JA, Drake C. “Medical Costs of Fatal and Nonfatal Falls in Older Adults.” Journal of the American Geriatrics Society. March 2018. Web. 27 September 2023.
20“Promoting Patient Safety.” Patient Safety Network. Web. 27 September 2023.
21Ulrich, R. S., Zimring, C., Zhu, X., DuBose, J., Seo, H. B., Choi, Y. S., ... & Joseph, A. 2008. “A review of the research literature on evidence-based healthcare design.” HERD: Health Environments Research & Design Journal. 2008. Web. 27 September 2023.
22Bae, S., & Fabry, D. (2014). “Assessing the relationships between nurse work hours/overtime and nurse and patient outcomes: Systematic literature review.” Nursing Outlook. March-April 2014. Web. 27 September 2023. < https://pubmed.ncbi.nlm.nih.gov/24345613/>
23Trinkoff, A. M., Johantgen, M., Storr, C. L., Gurses, A. P., Liang, Y., & Han, K. “Nurses’ work schedule characteristics, nurse staffing, and patient mortality.” Nursing Research. January-February 2011. Web. 27 September 2023.
24,25“Design Guide for Inpatient Mental Health & Residential Rehabilitation Treatment Program Facilities.” U.S. Department of Veterans Affairs. January 2021. Web. 27 September 2023.
26“Healthy Flooring.” Healthcare Without Harm.” Web. 27 Sept. 2023.
27“Design Guide for Inpatient Mental Health & Residential Rehabilitation Treatment Program Facilities.” U.S. Department of Veterans Affairs. January 2021. Web. 27 September 2023.
28Harris, D. D., & Detke, L. A. (2013). The role of flooring as a design element affecting patient and healthcare worker safety. HERD: Health Environments Research & Design Journal, 6(3), 95-119.
29Moussatche, H., & Languel, J. (2002). Life cycle costing of interior materials for Florida’s schools. Journal of Interior Design, 28(2), 37-49.
30,31,32“Design Guide for Inpatient Mental Health & Residential Rehabilitation Treatment Program Facilities.” U.S. Department of Veterans Affairs. January 2021. Web. 27 September 2023. <
33Butkovic, Marija. “6 Experts Weight In On The Present And The Future Of Mental Health.” Forbes. 11 July 2022. Web. 27 September 2023.
34“A Bridge Between Our Rich History and Future Opportunities.” National Alliance on Mental Illness. Web. 27 September 2023. https://nami.org/NAMInet/Board-of-Directors/Governance-Documents/NAMIStrategicPlan2020
Sandra Soraci EDAC, LEED AP, NCIDQ, is the Director of Healthcare and Senior Living Segment Strategy, for Tarkett NA. Sandra’s diverse and deep career-specific focus on healthcare and commercialization efforts fully informs the customer decision-making journey. Flooring is no longer a design feature, it is an investment in health and safety, and we all have a stake in improving outcomes for our customers. Healthy environments support the healing process, and that begins at the ground level, with the floor. Through an evidence-based design lens, Tarkett Flooring continually seeks to create flooring solutions that contribute to greater connection, safety, and overall well-being. Healthcare is ever-changing; my passion is to educate, elevate, and transform sales enablement to fully support what our healthcare customers tell us they need the floor to do.
Kathy Price-Robinson is a nationally known writer focusing on building and architecture. Her award-winning remodeling series ran 13 years in the Los Angeles Times. She has written for dozens of publications in the design and building industry and developed more than 100 continuing education.