Eight Fundamental Performance Characteristics of Healthcare Flooring Specification



Learning Objectives:
- Explain how flooring can help mitigate slips, trips, and falls (STFs), and have an actionable impact to lessen patient and staff injuries associated with falls.
- Discuss how flooring can reduce ambient noise levels and reduce staff fatigue in the healing environment.
- Describe how flooring choices can reduce surface contamination and potential risk of healthcare-associated infections (HAIs) as well as improve indoor air quality (IAQ).
- Identify how healthcare flooring can improve patient and family satisfaction as well as represent the best return on investment (ROI).
Credits:
This course is approved as a Structured Course
This course can be self-reported to the AANB, as per their CE Guidelines
Approved for structured learning
Approved for Core Learning
This course can be self-reported to the NLAA
Course may qualify for Learning Hours with NWTAA
Course eligible for OAA Learning Hours
This course is approved as a core course
This course can be self-reported for Learning Units to the Architectural Institute of British Columbia
Flooring sets the stage for all health care activities. Its aesthetics contribute to first impressions, a perception that shapes our opinion about the health system’s ability to provide safe, quality, and comfortable care.1
Health systems demand that their project partners evaluate, quantify, and provide them with flooring solutions that support total cost of ownership (TCO) given limited resources and capital dollars. Flooring is the foundation of the healing environment in that it supports all activities within the healthcare setting. Selection and specification decisions are best informed by credible evidence of performance characteristics and information extolled by flooring manufacturers. The paradigm of patient care has shifted. In order to meet the operational demands of the health system, architects, and designers understand it is more than just aesthetics; they strive to identify and validate how flooring performs for those who walk on it, heal on it, and maintain it.
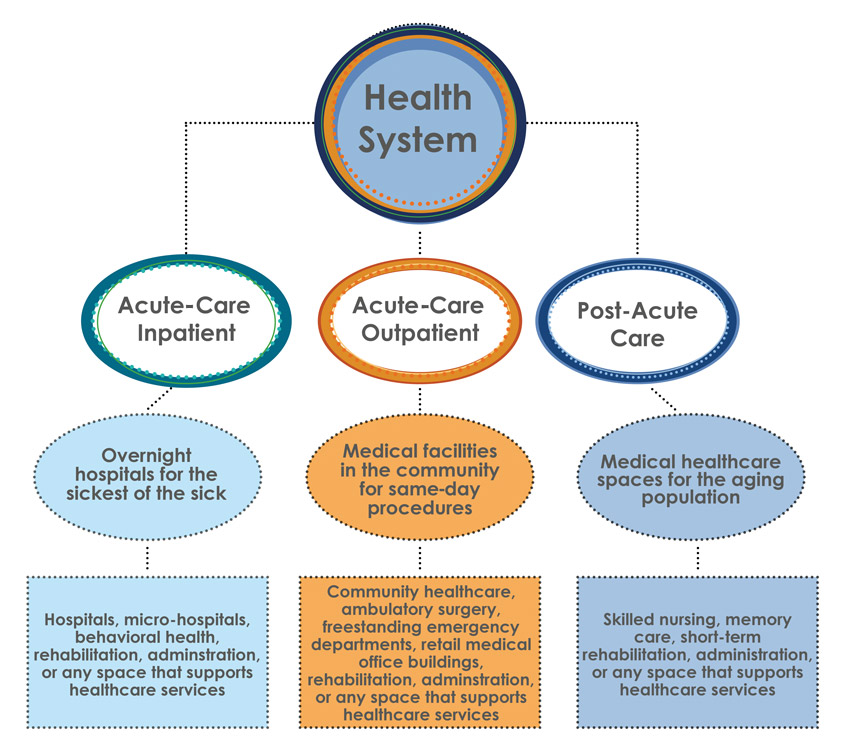
Image courtesy of Interface
We can categorize the three types of health facilities that are most commonly found in the United States to expand the reach and ease the burden on the health system as a whole. The Centers for Disease Control (CDC) defines healthcare setting to include but not be limited to: acute-care hospitals, outpatient clinics, physician offices and urgent cares, and long-term medical-based senior-care facilities.
Flooring is a complex, integrated system that consists of the subfloor, the floorcovering, and the surface finish, which, when combined, create a functional, durable surface for patient care, caregiver comfort, and operational and clinical efficiency. Client partners are demanding that their manufacturer partners provide a “complete flooring solution” for one point of contact to attain actionable outcomes and capture at-risk reimbursement dollars for the health system.
The Whole Building Design Guide (WBDG), a program of the National Institute of Building Sciences (NIBS), states: “A truly successful project is one where project goals are identified early on and where the interdependencies of all building systems are coordinated concurrently from the planning and programming phase.”2 Project drivers specific to flooring are examined during the schematic phase where performance characteristics are evaluated specific to the basis of design.
Human-centered design develops solutions to problems by involving the human perspective. In the healing environment, interior finish specifications focus on patient outcomes. The ability for patients to rest in quiet and hygienic surroundings, for maintenance teams to eliminate use of cleaning chemicals and turn over spaces quickly, and for caregivers to feel relief from foot, leg, and back pain from long shifts are just a few of the ways flooring holistically supports a health care setting.
EVIDENCE-BASED DESIGN AND ITSIMPACT ON HEALTHCARE FLOORING
According to The Center for Health Design, “Evidence-based design (EBD) is the process of basing decisions about the built environment on credible research to achieve the best possible outcomes.” EBD is a design objective that acknowledges the link between the physical environment, outcomes, and operational efficiency. In the built environment, architects and designers look to achieve project drivers through the EBD process.
“Evidence-based design (EBD) is the process of basing decisions about the built environment on credible research to achieve the best possible outcomes.”
—The Center for Health Design
In healthcare, flooring supports human-centered and evidence-based design. Great design is iterative (which is the repetition of a process in order to generate a sequence of outcomes), and the human-centered approach to product selection must address human need, cognitive empathy, creative possibilities, and support real outcomes, such as economics, TCO, operational optimization, health and safety impacts, and environmental considerations.
EBD takes into consideration the comprehensive and holistic influence buildings have on their occupants, health outcomes, infection control, and acoustics and underfoot comfort. Both human-centered design and EBD incorporate several factors that emphasize wellness for the building occupant. Healthcare’s space-specific needs drive specification of flooring based on project drivers, the population it serves, and the building occupants. By emphasizing EBD goals, the findings can be used by architects and designers to prioritize and identify the performance characteristics of the floor best suited to achieve the desired outcomes. Good design acknowledges that rather than offering a prescription for floor-covering selection, an evidence-based tool should be utilized to inform design decisions.3
HEALTH CARE REIMBURSEMENTS AND PATIENT SATISFACTION
The specification of a flooring product that contributes to better patient satisfaction can have significant financial implications. The patients’ perception of their hospital experience is measured by the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) scores, which is a patient satisfaction survey required by the Centers for Medicare and Medicaid Services (CMS) across acute-care hospitals in the United States.4

Image courtesy of Interface
The Hospital Value-Based Purchasing program is a Center for Medicare & Medicaid (CMS) initiative that adjusts what Medicare pays hospitals under the Inpatient Prospective Payment System (IPPS) based on the quality of inpatient care the hospitals provide to the patient (www.cms.gov).
CMS funding is tied to patient experience, outcomes, safety, falls, infection, and noise. Therefore, it is essential to specify flooring that is informed by EBD and supports operational optimization for the health system’s bottom line. It is also important to assess the flooring’s ability to have an actionable impact on reimbursement drivers supported by the impact of EBD in health care.
EBD FLOORING PERFORMANCECHARACTERISTICS
The Center for Health Design (CHD) identified eight performance characteristics that define the impact flooring has on operations, health, safety, and wellness.5 The characteristics are based on an EBD approach to define how flooring can contribute to the following performance improvement goals:
- Reduce slips, trips, and falls (STFs).
- Reduce patient and staff injuries associated with falls.
- Reduce noise levels.
- Reduce staff fatigue.
- Reduce surface contamination and potential risk of healthcare-associated infections (HAIs).
- Improve patient and family satisfaction.
- Improve indoor air quality (IAQ).
- Represent the best return on investment (ROI).
The eight performance characteristics for flooring as it relates to EBD clearly show that specifying the right flooring, to address space-specific needs can have an actionable impact on patient outcomes and TCO to support a positive healing environment with a durable, aesthetic, and functional surface for decades to come.
Let’s look at each of the eight performance characteristics individually.
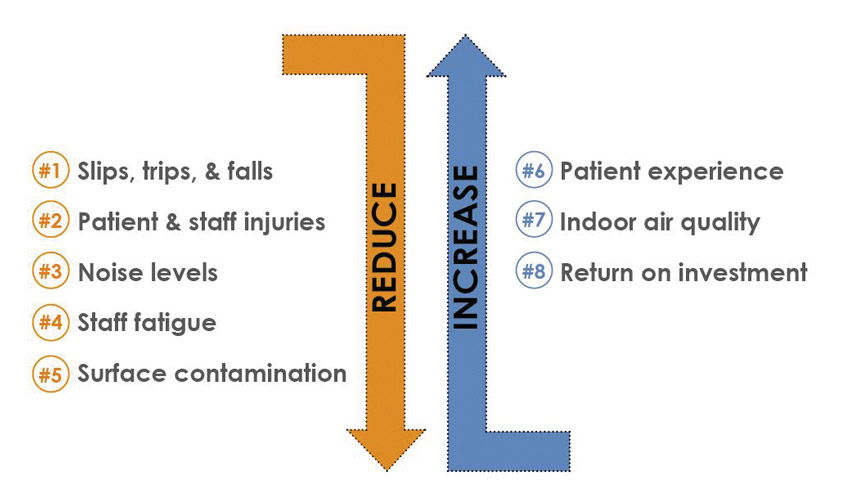
Image courtesy of Interface
There are eight performance characteristics to evaluate how flooring/floorcoverings can contribute to outcomes as defined by the CHD study.
EBD PERFORMANCE CHARACTERISTIC #1: REDUCE SLIPS, TRIPS, AND FALLS (STFS)6
In every healthcare facility, safety is paramount when it comes to flooring specification and performance characteristics. Falls are a common and devastating complication of patient care, particularly in elderly patients. Studies have found that falls occur at a rate of three to five per 1,000 bed-days, and the Agency for Healthcare Research and Quality (AHRQ) estimates that 700,000 to 1 million hospitalized patients fall each year.7 A fall is considered a “never event,” which means it should never happen and is non-reimbursable to the health system. Resilient flooring with an extremely dense, never-coated surface delivers the best coefficient of friction (COF) to reduce STFs. It is important to understand that the COF can be negatively altered on a coated or waxed resilient floor. The emphasis of flooring safety is to mitigate STFs and facilitate the transport of rolling loads over a level the floor surface without transition strips. Compliant flooring is a passive intervention approach designed to reduce the stiffness of the ground in order to attenuate the impact forces applied to the body. In the event of a fall, it has the potential to reduce the incidence and severity of all fall-related injuries caused by impact to the ground, including hip fractures and traumatic brain injuries.8,9,10,11,12
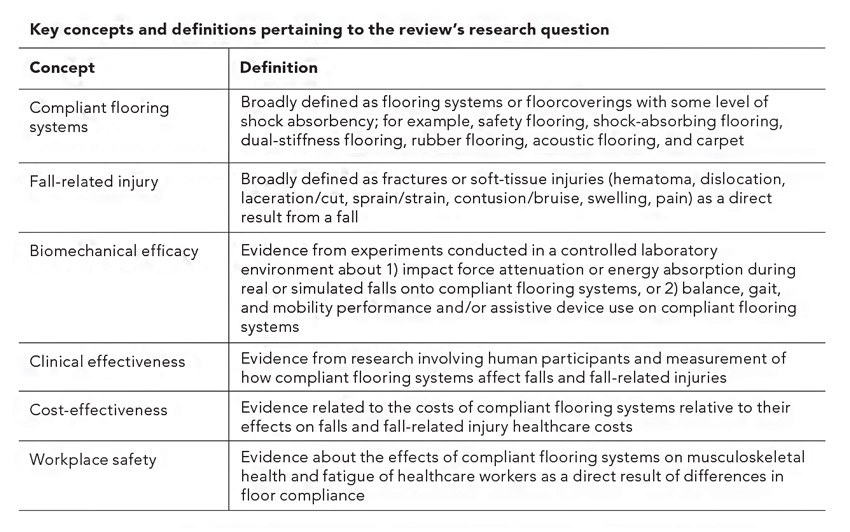
Source: Lachance, Chantelle C. et al. “Compliant flooring to prevent fall-related injuries: a scoping review protocol.” BMJ Journals.
Shown are the key concepts for complaint flooring: slip, trip, and fall.
The Facilities Guidelines Institute (FGI) Guidelines for Design and Construction of Hospitals, 2018 Edition states that some studies suggest that flooring with a medium-sized pattern (1 inch to 6 inches wide) were associated with more falls than floors with no pattern, a small pattern (less than 1 inch wide), or a large pattern (wider than 6 inches). For floor contrast, high-contrast patterns on floor surfaces may be associated with more patient falls, especially with glare.
In regard to floor reflectivity, finished floors (coated or waxed) with a high gloss value cause glare that may compromise patient vision, disrupting balance. The selection of non-wax or never-coated resilient flooring eliminates finish glare. Where a finish coat is required, smooth flooring surfaces should be sealed with a matte finish to reduce surface glare. Additionally, glare emitted from a coated or waxed resilient floor can alter cognitive perception, affect visual acuity, and be a potential trip hazard. Glare becomes more of a problem as we age, and a finish with a low reflectance value prevents glare.13 According to the American Optometric Association, changes in the lenses in aging eyes cause light entering the eye to be scattered rather than focused precisely on the retina.14 A never-coated floor mitigates the risk of STFs that can be present on a wax-coated surface.
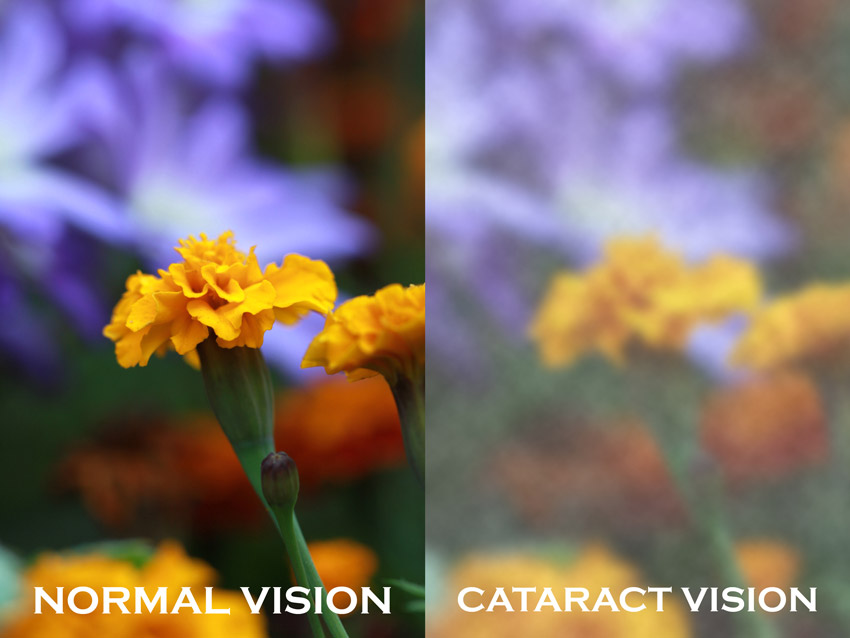
Image: www.carelinx.com/blog/aging-eyes-major-vision-loss
Changes in the lenses in aging eyes cause light entering the eye to be scattered rather than focused precisely on the retina.
When it comes to carpet tile, the dense fiber construction can reduce instances and severity of slips and falls. Specifically, the Americans with Disabilities Act (ADA) discusses COF requirements in Appendix A4.5.1: “The Occupational Safety and Health Administration (OSHA) recommends that walking surfaces have a static COF of 0.5. A static COF of 0.6 is recommended for accessible routes and 0.8 for ramps.”
In addition, a continuous flooring solution will minimize surface transitions. The FGI Guidelines states that smooth transitions shall be provided between different flooring materials; Section A2.1-7.2.3.1 (3) states that flush thresholds should be used to reduce tripping hazards and push/pull concern.
Look for a system that can integrate different flooring solutions, such as premium rubber, luxury vinyl tile (LVT), and carpet tile with minimal surface transitions. To best achieve the goal of safety for patients and caregivers, specify flooring that has an actionable impact on STFs and associated injuries.
EBD PERFORMANCE CHARACTERISTIC #2: REDUCE PATIENT AND STAFF INJURIES ASSOCIATED WITH FALLS17
According to OSHA, STFs account for 15 percent of all accidental deaths (some 12,000 a year).18 STFs are among the most frequently reported injuries and account for 25 percent of reported workers’ compensation claims per year. Falls result in more than 2.8 million injuries treated in emergency departments annually, including over 800,000 hospitalizations and more than 27,000 deaths.19 The operational costs for fallers with serious injury increases length of stay by 6.3 days.20 This cost must be absorbed by the health system, as these occurences are considered ‘never events’ and non-reimbursable.20
The Safety Risk Assessment (SRA) Toolkit v.2 from The Center for Health Design evidences a proactive process that can mitigate risk, a discussion prompt for a multidisciplinary team EBD approach to identify solutions. The SRA targets six areas of safety: infection, falls, medication errors, security, injuries of behavioral health, and patient handling. Falls is one of the six areas required in the 2018 FGI Guidelines.21
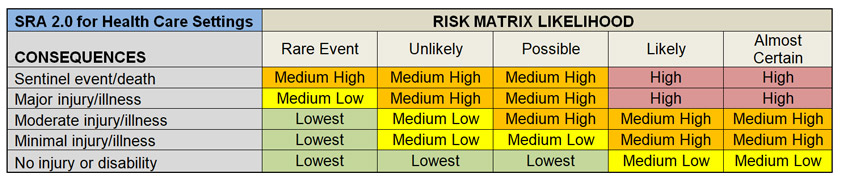
Source: The Center for Health Design
The SRA 2.0 for healthcare settings risk matrix shows the likelihood of consequences resultant from a fall.
Performance characteristics of flooring are often overlooked for the actionable impact they provide as it relates to STFs. Specifying resilient flooring with a high COF, a continuous level surface, and that does not require coatings or wax is consistent with providing an environment that minimizes the risk of STFs.
Assessing the influence of floorcovering compositions on reducing ground impact force from falls, providing firmness and stability to prevent trips and loss of balance, increasing slip resistance, and reducing rolling resistance to minimize manual wheelchair pushing effort could be immeasurable in improving quality of life and reducing the economic impact of injuries most often seen in these populations.
The FGI Guidelines indicate that the subfloor, the composition of a flooring material, and the material’s ability to yield to pressure should be considered when selecting flooring that can contribute to force attenuation when a fall does occur.
Notice



