Using Ventilation Systems to Limit the Spread of Airborne Infections



Single-Source Infection Control
Do hospital-acquired infections thrive in part because we are already dividing and diluting our opposing forces?
Within a hospital facility, there is the environment health and safety (EH&S) department, medical equipment management department, custodial department, and O&M department, to mention just a few, all with their own infection control (IC) responsibilities. These groups collectively share a portion of the hospital’s IC responsibilities. Unfortunately, each is a silo in itself, and while hospital acquired infections (HAI) have been reduced in recent years and IC policy and procedures have improved along with record keeping, HAIs have not been eliminated and will not be eliminated while individual health care silos exist.
So, let’s tear down the silos. Let’s outsource all tasks associated with cleaning and caring for IC prevention to a for-profit HVAC maintenance company that will set up a single-source IC work order system, with the work completed by technicians trained in IC maintenance. Why the HVAC department? Because this support service group is proficient in maintaining and caring for equipment systems and material through the use of preventive maintenance work orders. What other hospital group has a work order system?
This article will address the need to “break the mold” by taking infection control management (ICM) from the clinical side of the hospital and placing ICM into the hands of a high-performance support service group. To be more specific, we are suggesting this hybrid department consist of personnel drawn from each of the health care department roles (custodial, medical equipment, etc.), and then train this cross-trained group to be the outsourced, for-profit ICM maintenance company that comes in to focus solely on IC and nothing else.
Instead of further decentralization of ICM to individual departments, such as the operating rooms, cesarean section, etc., centralizing ICM will capitalize on time-tested quality control processes where a single-source group’s sole responsibility is to assure optimum IC maintenance results. Integral to this approach will be the uses of a computerized maintenance management system (CMMS) system to methodically task the work, complete the work, spot-check work order completion accuracy, and report on IC maintenance work order performance. With outside financial penalties hanging over health care facilities, high-performance ICM can be better achieved through efficient work order management and record-keeping dedicated solely to IC hygiene and its prevention of HAI. It is time for a change for the sake of all those people entering a health care facility and not for the retention of silos.
Medical personnel’s primary responsibility is to care for patients and not to manage IC P&P or complete IC work orders. Health care facilities continue to struggle with eliminating HAIs because the most qualified individuals to be completing these IC tasks are not always the ones performing the ICM work.
Another example of the disconnect within a building is the custodial/housekeeping and HVAC preventive maintenance. These two departments have different department heads, and each goes about his or her work using different metrics to achieve results. The foundation for a single-source department is the commitment to quality control followed with the uses of an IC computerized work order system that combines clinical department hygiene procedures, custodial hygiene procedures, environment hygiene procedures, and mechanical/electrical hygiene tasks as they pertain to routine maintenance that can be completed, measured, and subject to continuous improvements. A single IC work order system can provide consistent measurement metrics that currently are not being incorporated through silo management.
This sole-source initiative will include a team of specialists trained to focus on IC-specific areas within housekeeping, medical equipment, HVAC temperature and humidity, air changes, filter replacement, etc. The driving force will be the “for-profit” performance. Analogous to the pharmaceutical industry, where the product going out the door must have “zero defects” because recalls cost money, the health care industry needs to mirror what the pharma business is doing to assure peak IC performance that reduces the billions of dollars lost world-wide each year to HAI.
Back in the 1990s, the phrase “zero defects” enjoyed a renaissance as an integral part of quality control embraced by endless numbers of companies in numerous industries. Zero defects should be the mantra for eliminating HAIs and the watchword for this new, single-source ICM group within each health care facility.
One CDC estimate has stated that one in 25 hospital patients get an HAI while being treated in a medical facility. While clinical procedures and protocol strive to work in conjunction with the building management support services, HAIs continue to thrive, and a radical change should be considered based on a few concepts (courtesy of Philip B. Crosby’s Four Absolutes of Quality Management):
- Quality is conformance to requirements;
- Quality comes from prevention;
- Quality performance standard is zero defects; and
- Quality measurement is the price of non-conformance.
I personally observed a family member becoming one of the 25 patients with an HAI while being treated in a hospital. This patient passed away a month later due to HAI complications. What struck me with each visit I made to this major hospital was how proficient nurses were with the use of a bar code scanner to capture the cost for each pill, medication, etc. given to the patient. You could say this was a for-profit initiative. At the same time, these aides did not conform to IC requirements when entering and leaving a patient room. HAI prevention was not avoided in the case of this family member, and zero defects were not achieved.
Based on my previous quality control training at a design-build HVAC firm and the Center for Quality Management training (Cambridge, Massachusetts) I received in the early 1990s, I am of the opinion that those departments with IC hygiene responsibilities should abdicate these tasks to a stand-alone ICM group that is a branch of an HVAC maintenance outsourced firm.
Integral to this transfer of responsibilities will be the transfer of certain existing employees from their current departments to this outsourced company. Trained in quality control, the vision will be to achieve IC zero-defects. Due to the seriousness of HAIs, I would suggest that this ICM-HVAC maintenance company answer to the president of the hospital. The “cold-cash” fact of HAI is that this health care problem affects a hospital’s bottom line. Far worse is the devastating effects that HAIs cost with the loss of thousands of patients while in a medical facility as well as the less-documented death of individuals from HAIs after they have left the hospital and the resulting impact it has on family and friends.
ICM Organization and Process
The establishment of an ICM maintenance department begins with volunteers from the outsourced company, in-house medical staff, and a third-party IC consultant joining a solution team steering committee. The steering committee will oversee the problem-solving quality control initiative set back in the 1900s when Walter Shewhart, engineer and statistician, formulated the Shewhart Cycle, or “Plan-Do-Check-Act.” This cycle flow diagram combined with Jiro Kawakita’s W-V model provided teams a roadmap to achieving zero defects. It is this zero-defect focus that is needed to eliminate HAIs today, and who is better qualified than a single-source group experienced in completing IC hygiene work orders?
Quality control professionals learn from the W-V diagram that one does not jump to the solution. First, data has to be collected and analyzed. That is not clearly stated in the joint commission, Chapter 3, “Assessing Risk,” which states, “The assessment is the foundation of every organization’s infection prevention plan.” Assessment is not the same as “analyze the data” followed by “solution planning.” The same can be said for Chapter 3’s comment, “The risk assessment should serve as the basis for developing written goals.” Only through solution planning and solution implementation can goals be set and solutions measured.
In parallel with solution planning and solution implementation, an ICM maintenance organization chart can take form via development of job descriptions and IC hygiene-specific work orders.
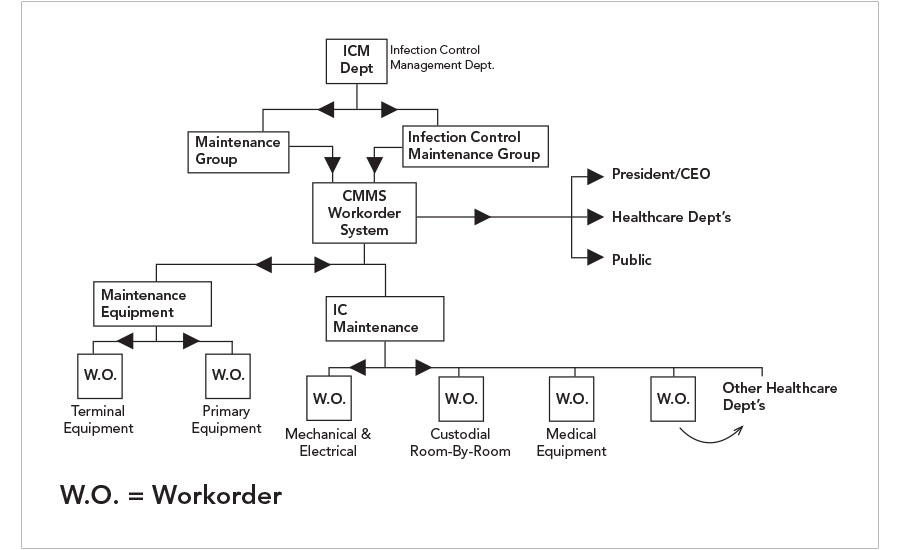
Image courtesy of Building Smart Software
FIGURE 1. Proposed organizational chart incorporating a dedicated Infection Control Management department.
The means-to-measure performance will come out of the solution planning and implemented as the solution(s) is/are executed. Based on the measured success of the solution, IC hygiene can progressively eliminate HAIs from the facility and sustain zero defects.
The cornerstone to successful ICM will be the CMMS system populated with standardized work order tasks; timeline to complete the tasks; means to measure the work; and, of course, the results. Using the IC hygiene work order system, IC cleaning is completed, documented, analyzed, measured, benchmarked, and continuously improved upon by the entire ICM staff. Results and recommendations can be made to the other departments within the hospital from the ICM performance. With these work orders completed and HAI incidents measured, the improvements can continuously enhance solution(s), return on investment from ICM can determined, and further problem-solving can addressed through lessons learned. This IC database shall include clinical equipment, room/custodial, mechanical and electrical equipment, IC policy and procedure reporting, completed work order reporting, IC complaint and resolution reporting, and quarterly report to pertinent departments and administration as well as to the public.
The benefits of a work order system are:
- A standardized checklist of things-to-do;
- A means to monitor and verify work performed;
- A method to collect, analyze, and report on work order success;
- A means to update and continuously improve IC hygiene management; and
- A method to compare past-to-present results and publish the IC improvements.
In addition, ICM “story boards” highlighting the hospital’s success can be posted in public spaces to advertise the facility’s initiatives just as pharma facilities do to raise employee and public awareness. This ICM work order system eliminates finger-pointing because the work is performed by a group of IC specialists with a single focus in IC hygiene.
Without jumping to the solution before this analytical process above has been completed, it is suggested this new ICM group take full responsibility for IC success. A manager trained in IC as well as O&M and work order systems will head the department. The group will have an experienced IC trained CMMS operator to populate the work order system database. In addition, experienced personnel from other departments will join this group to fulfill IC specific tasks in housekeeping of all rooms, not just special rooms, e.g., intensive care units and operating rooms. ICM will be responsible for medical equipment, HVAC criteria (temperatures, humidity levels, space pressure, air changes), and other trades.
Summary
Hospitals should establish a for-profit IC support service group located in the health care facility by following these steps:
- Create a “solution team” to brainstorm how IC management and the IC P&P could be implemented using personnel and a CMMS system.
- Restructure the job description into an ICM department head, CMMS operator, and IC technicians to perform the work order system in accordance with the group’s policy and procedure.
- Create an organizational chart to shape the ICM group drawing upon other support service groups (e.g., HVAC department) to join in the IC responsibilities as well as retain an outside IC health care specialist third-party adviser for guidance.
- Create an ICM budget, drawing upon previous department budgets for IC that were managed by various other groups in the hospital. Redistribute this budget based on the new ICM outsource firm.
- The solution team will remain intact as a third-party oversight committee monitoring and meeting quarterly with the ICM company to continuously improve the IC process.
This ICM approach is an abbreviated discussion of finding a better way to improve IC and achieve zero defects within a medical facility, but it is based on time-test quality control methods used for problem solving to continuously improve a process as well as troubleshoot a chronic problem. In the real world, hospitals will most likely be too bureaucratic to give up infection control tasks with each management silo. However, breaking the mold (no pun intended) and thinking outside the bureaucratic box by just one health care facility would be a positive first step.

|
Howard McKew, P.E., FASHRAE, is the president of Building Smart Software. |
| Engineered Systems (ES) Magazine promotes energy-efficient solutions for high-performance buildings by offering insights and news for mechanical consulting and facility engineers. ES authors draw from current trends and practical successes in the design, maintenance, and commissioning of HVAC and building automation systems. Whether for a retrofit or new construction, ES delivers new ideas to help your commercial, institutional, mission critical, and government buildings achieve LEED and Energy Star certification. ES is written by engineers for engineers. |
Notice



