Creating Healthy Healthcare Environments
The choice of products can affect the health of staff and patients in healthcare facilities
![]() Continuing Education
Continuing Education
Use the following learning objectives to focus your study while reading this month’s Continuing Education article.
Learning Objectives - After reading this article, you will be able to:
- Identify and recognize the health issues related to the transfer of infectious bacteria in indoor healthcare environments.
- Investigate the options and alternatives to improvement in healthier environments that contribute to indoor environmental quality in LEED and in general.
- Compare and contrast the differences between chemical approaches and natural approaches to addressing infectious bacteria in LEED-certified buildings and others healthcare facilities.
- Specify natural antimicrobial flooring and wall material consistent with LEED v4 for Healthcare.
Patients generally tend to think of a healthcare facility as the first step on the road back to wellness. However, healthcare professionals, architects, and designers are becoming increasingly aware of a darker truth: The healthcare environment can create toxic threats to people, making them a short cut to more serious illness, permanent harm, and even death. And the risk isn't only limited to hospitals, but to other healthcare buildings where many people are brought together including all types of care facilities, acute care centers, specialty hospitals, clinics, ambulatory surgical centers, and long-term care facilities. The first step in creating truly healthy environments is to recognize the problem and then to find the most appropriate means of addressing it.
A Growing Problem: Hospital-Acquired Infections
The means of transferring illness from one person to another in an indoor setting is contained in infectious bacteria. It is these bacteria that are deposited on surfaces typically from an already infected person. When a non-infected person comes in contact with the bacteria in the indoor environment they are prone to have it transferred to something they are eating or drinking or to enter their body directly when they rub their eyes or nose, so they can become infected as well. This simple but common means of transferring infectious bacteria, and thus illness, is becoming increasingly recognized as a problem in indoor environments. Of particular concern is a growing realization that hospital patients are being infected with diseases from this bacteria while they were still in the hospital thus giving rise to the term hospital-acquired infections (HAIs).
Numerous studies have calculated the impact of these HAIs identifying as many as one in 20 patients who will contract an HAI sometime during a hospital stay. While it's bad enough that these hospital patients are getting infected and ill, what's worse is that four in every 100 will die. That's more than the number of Americans killed in car accidents, fires, and drowning combined. Hence, HAIs are currently recognized as being among the most common causes of accidental death in the United States.

Photo by Stantec/Halkin Architectural Photography LLC; courtesy of Forbo Flooring Systems
Children’s Specialized Hospital in Mountainside, New Jersey
In response to these serious concerns, healthcare professionals worldwide are becoming increasingly focused on creating environments that fulfill the fundamental tenet at the heart of every physician's Hippocratic Oath: Primum Non Nocere—first, do no harm. Architects and interior design professionals share in this focus in that we are obligated to protect the health, safety, and welfare of the public. While we also do not seek to do any harm to people, we have the means to find ways that improve the indoor environment to be truly healthier and safer, particularly to vulnerable populations such as hospital patients. Most architects and designers are already aware that indoor air is often contaminated with a complex mixture of chemicals from many sources, including emissions from building materials. Disease risks in people related to this polluted environment can include asthma, bronchitis, cancer, and reproductive, developmental, and neurological disorders. Hence it has become the norm to specify and design with building materials and products that avoid these emissions or contaminants in the interest of creating safer, cleaner indoor environments. We have the opportunity to act in a similar way regarding HAIs.

Photo by Brian Dressler Photography Inc.; courtesy of Forbo Flooring Systems
The Patewood Memorial Hospital in Greenville, South Carolina, used linoleum flooring that contributes to a positive life-cycle assessment for buildings.
Hospital administrators and staff have also taken on the quest to create safer indoor environments by using cleaning routines that include powerful new antibacterial compounds developed to fight off infectious bacteria. The good news is that healthcare workers are beginning to make progress against two of the best-known infectious bacteria namely MRSA and Clostridium difficile (C. difficile). Government data from Public Health England reported that better control of MRSA and C. difficile led to a nationwide decrease in the prevalence of HAIs from 8.2 percent in 2006 to 6.4 percent in 2011. The bad news is that many other bacteria have reacted to those antibacterial compounds by mutating to resist them. A new wave of treatment-resistant bacteria is now emerging which includes Carbapenem-Resistant Enterobacteriaceae (CRE) and multidrug-resistant Acinetobacter. These new, mutated, treatment-resistant bacteria, referred to as “super bugs,” combine a high mortality rate with resistance to nearly all contemporary antibiotics. With newer disinfectants and antibiotics being created to address this issue, the bacteria are likely to mutate again and escalate this form of biological warfare even further. Paradoxically, infection control professionals are also seeing a rise in the incidence of hospital-based infection from more common bacteria, from coliforms like salmonella and E. coli to treatment-resistant strains of tuberculosis.


Photos courtesy of Forbo Flooring Systems
In response to the fight against hospital-acquired infections (HAIs), hospital staff have commonly increased cleaning regimens to include disinfectants that can lead to mutated bacteria that are resistant to treatment.
In addition to enduring the use of these aggressive disinfectants, healthcare professionals are forced to function in an indoor environment filled with toxic disinfectant chemicals that are bound to impact patients and caregivers alike. Further, the cost of implementing this type of infection control becomes an escalating burden on already overtaxed healthcare budgets. In fact, research recently released by JAMA Internal Medicine reported that HAIs cost $9.8 billion every year. This report has understandably received an enormous amount of attention in an era where healthcare cost savings are constantly in the news.
Industry Response: Antimicrobial Chemicals

Blanchard Valley Regional Medical Center, Findlay, OH, photo by Marquart Architectural Photography; courtesy of Forbo Flooring Systems
In addition to patients, healthcare staff who may work for years in hospitals and other facilities are at increased risk from environmentally acquired diseases.
While cleaning and disinfecting will likely always be part of an appropriate plan to fight off infectious bacteria, other approaches have been investigated as well. One of the more common strategies is to specify products, such as fabrics and flooring, that are treated with chemicals that act as antimicrobial agents to prevent bacterial growth. Unfortunately, this solution creates more problems than it solves since the chemicals used to make these products anti-microbial are commonly classified as pesticides or biocides. That means that the added antimicrobial chemicals include harmful contaminants that are innocently being introduced into indoor environments although their long-term health effects are largely not known by designers, building owners, and maintenance professionals. However, a half century of experience with the environmental impact of pesticides teaches us that indiscriminate and/or excessive pesticide use can threaten more than just pests. It has been proven that these chemicals accumulate in our bodies over time such that regular small doses can be just as troubling as a large single dose. The danger is imminent—so much so that the European Union put a set of restrictive new rules on the use of biocides in place in 2012.
In this country, the U.S. Environmental Protection Agency (EPA) has gone a step further and identified persistent bio-accumulative and toxic (PBT) materials and indicated that they should clearly be avoided. Scientists are investigating the causal links between PBTs and pesticides and the increased incidence of several types of diseases. These diseases include asthma, allergies, and other respiratory diseases plus the proliferation of other chronic health consequences, including cancer, birth defects, neurological and reproductive disorders.
Adding insult to injury, there is another issue with antimicrobial chemicals added to products—they don't actually kill off bacteria. Instead, they typically prevent the bacteria from growing beyond whatever level already exists. That is good and desirable, but not when it relies on pesticide and biocide-based chemicals. The combination of remaining infectious bacteria and the added negative health effects of the added chemicals has been linked to a growing wave of chronic diseases that are hitting hospitals, clinics, and care centers nationwide.
Indoor Environmental Quality Issues
In the last half of the 20th century, according to the United Nations' Millennium Ecosystem Assessment, humans have changed their ecosystem more rapidly and extensively than in any comparable time in human history. The creation of a resultant “chemical society” has been a long-term concern of governments worldwide. In 1995, the United Nations called for global action to remove persistent organic pollutants (POPs) from our environment. The worldwide Stockholm Convention created an international treaty aiming to eliminate POPs from production and use. Unfortunately, the United States is one of only seven nations worldwide that has failed to ratify the treaty yet.
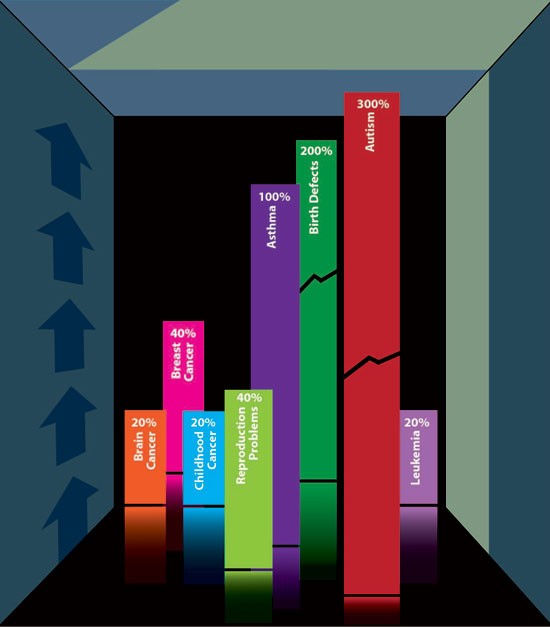
Chart courtesy of Forbo Flooring Systems
Studies are finding an alarming rate of links between increases in chronic diseases and the built environment.
The consequences of ecological change and increased presence of chemical pollutants are starting to be associated with alarming increases in chronic diseases. The jump is particularly pronounced in diseases that have suspected links to hazardous chemicals present in building materials like vinyl flooring, wallpaper, and other products that use polyvinyl chloride (PVC). Numerous studies have shown PVC to be the single largest material source of dioxin to the global environment over the course of its life cycle including production, use, and disposal. Diseases linked to this exposure include childhood leukemia, brain cancer, and other childhood cancers that have increased by more than 20 percent since 1975. Studies have shown that the birth of males with undescended testicles has increased 200 percent between 1970 and 1993. In women, breast cancer rates increased by 40 percent between 1973 and 1998 and 40 percent more women had difficulty conceiving a child in 2002 than in 1982, with a particularly sharp increase in reproductive difficulty among younger women ages 18–25. In general, asthma was twice as common in 1995 as it was in 1980 and autism spectrum disorders have become 10 times more frequent today than in the 1990s. These health facts are becoming increasingly difficult to ignore. Levels of bio-accumulative phthalates, dioxins, mercury, lead, and cadmium used in our built environment must be addressed. The need is becoming more profound as we create indoor environments that are more airtight in the name of energy efficiency. This trend is especially significant in healthcare environments, which are filled with patients whose diseases could be aggravated by environmental toxins.
While patients may be the focus of a healthcare environment, doctors, nurses, and other medical professionals are equally at risk. Surprisingly, very little has been done to protect U.S. health professionals from exposure to hazardous chemicals in their indoor environment. Some of these professionals have become concerned enough about the lack of control over chemical exposure that they have created an organization called Healthcare Without Harm (www.noharm.org). In the stated view of a representative of this global coalition of hospitals and healthcare systems, “by using excess energy, polluting the environment with phthalates, mercury, and other toxic chemicals, and producing waste which is burned rather than recycled, healthcare is ultimately compromising public health and damaging the ability of future generations to meet their needs.” Related to the burning of medical waste and other materials containing toxins, it is important to remember that quite often when toxins go into an incinerator it often means toxins come out of an incinerator. Fortunately, their message is getting through as they pursue improvements to hospital, clinic, specialty care and long-term care interior environments. One bright spot is the agreement to eliminate the use of any PBT phthalates, a class of chemicals used to make polyvinyl chloride (PVC) plastics flexible. These chemicals have been specifically targeted since they pose specific, identifiable threats to occupants of healthcare environments. Studies of phthalate exposure in the hospital setting point to the possibility of retarded sexual development among babies with high blood phthalate levels. A larger threat exists for healthcare workers who can often experience heightened phthalate exposure over many years, leading to the potential for allergies, cancers (especially breast cancer), and endocrine disruption, plus a host of other risks from obesity and diabetes to liver disease and infertility.

Photo by Fred Gerlich Photography; courtesy of Forbo Flooring Systems
McLeod Health Systems in Florence, South Carolina
The good news is that the products to solve the problem are already in the marketplace. PBT phthalates can be readily eliminated from an interior environment by choosing from the alternate, existing, and available building products that have never contained them and will never need to. All we need is the willingness of building designers, facility owners, and maintenance professionals to put them to use.
An Alternative Green Response: Natural Materials
While the larger problems of bacterial infestation and indoor environmental health may not lend themselves to quick, easy solutions, some steps can create an immediate improvement. Recognizing that there are alternatives to toxic or polluting solutions, the U.S. EPA has recommended that hospitals and other institutional or commercial facilities adopt an Integrated Pest Management (IPM) program to fight the super bug scourge. The IPM approach balances the need for effective control of hazards with a more global concern for the healthiness of everyone impacted, from patients and caregivers to beneficial microbes and bacteria. Three key steps are commonly part of an IPM program:
Prevention Rather than Poisoning
The EPA's approach focuses on investing time and effort to minimize risk, rather than reacting to preventable threats after they arise. The goal is to avoid surfaces that promote bacterial growth, to disinfect surfaces more frequently with milder cleaners, and to encourage activities (like hand washing and cough etiquette) that reduce the likelihood of transmitting infection.
Focus on Natural Alternatives
The EPA acknowledges that many products that tout themselves as antimicrobial are actually impregnated with chemical pesticides or biocides that can jeopardize the health of a vulnerable healthcare population. A good first move is to replace products that add to the problem with ones that reduce the risk naturally, without the need for toxic chemical additives or expensive installation or maintenance procedures. The use of natural materials which can naturally inhibit bacterial growth without additives can achieve the same result without exposing patients and healthcare givers to the risks of pesticides and their bio-accumulative toxicity.
Setting an Action Threshold
It is virtually impossible to totally eliminate bio-based risks, so the wiser strategy is to set an acceptable level of sanitation and maintain it consistently. This allows facility managers to sustain a healthful environment without expending vast resources to achieve a marginally negligible improvement.
When following this IPM approach and looking for alternatives, it is important that those alternatives are well understood. Recognizing that PVC has been identified as a material to avoid, many well-meaning design professionals consider substituting “rubber” alternatives for PVC-based products. While believing rubber to be a more natural product, the truth is that the vast majority are synthetic rubber products with little to no natural rubber content. While they do not emit phthalates, they contain other Chemicals of Concern in significant amounts. For example, studies done by the European Resilient Flooring Manufacturer's Institute (ERFMI) indicate the overall environmental impact of synthetic rubber flooring is substantially worse than that of PVC. If you want to avoid toxic chemicals, combat global warming, and save scarce resources, PVC is a poor choice. Synthetic rubber products can be an absolutely disastrous one. The Resilient Floor Covering Institute (RFCI) recently published product category EPDs indicating that all rubber products in the United States have a binder of only 0.6 percent natural rubber, with the balance being synthetic rubber (http://www.rfci.com/environmental-product-declaration/rubber-floor-tile/).
Photo courtesy of Forbo Flooring Systems
The manufacturing process of linoleum relies on natural ingredients and a concerted effort by manufacturers to reduce the amount of energy used in the process.
Linoleum: A Natural Alternative
When selecting or specifying materials and products in buildings, architects and designers have many other choices. Those choices can be beneficial to the indoor environment or not. We will use flooring as our primary example here to demonstrate that it is one of many products that can be selected using the principles discussed thus far to create safer, healthier, indoor environments.
There are a number of flooring choices besides PVC or synthetic rubber products. Among them is a sometimes overlooked choice in linoleum. First invented in 1860 linoleum has always been considered to be an excellent, inexpensive material for high use areas. In the late nineteenth and early twentieth centuries, it was favored in hallways and passages, and as a surround for carpet squares. However, many people may still associate linoleum with its common mid-twentieth century use on kitchen and bathroom floors. Its water resistance enabled easy maintenance with readily sanitary cleaning while its resilience made standing on it easier on the body. From an aesthetic standpoint, it offers a range of colors and artistic options. In fact, early in the twentieth century, a group of artists including Pablo Picasso and Henri Matisse created works of art out of linoleum by adapting the printmaking techniques for woodcut prints to linoleum, thus creating the linocut printmaking technique.
The linoleum production process has existed for more than a century. It is a craft which essentially consists of oxidation, mixing, calendaring and drying the various ingredients into a finished product. The ingredients used are in fact all natural and mostly bio-based including the following:
• Rosin, the key agent in the first steps of producing linoleum is tapped from pine trees, usually without affecting growth. Together with linseed oil, rosin gives the finished product its strength and flexibility.
• Linseed oil, the most important raw material used to make linoleum, is obtained by pressing the seeds of the flax plant. In the past linseed oil was used as cooking oil, as well as for lighting. Adding tall oil, a recycled post-industrial by-product of the kraft paper industry, optimizes the oxidation process in the production of linoleum.
• Wood flour is used to bind the pigments and to ensure colorfastness meaning that linoleum is able to keep its vibrant colors throughout its lifespan. Another reason for using wood flour is that it helps to give an especially smooth surface. Some manufacturers have chosen not to use tropical hardwood flour, instead using wood flour made from timber grown in controlled European forests, where every tree felled is replaced.
• Cork flour is made by grinding the bark of the cork oak, which is grown around the Mediterranean. The bark is peeled off every seven to ten years without affecting the tree's growth. Cork flour is used as a raw material in some linoleum products.
• Limestone, when very finely ground, is a valuable ingredient for the strength of linoleum products. It is found all over the world in enormous quantities.
• Pigments are selected to create a wide range of attractive colors. By using ecologically responsible pigments that do not contain heavy metals such as lead and cadmium, manufacturers keep linoleum free of harmful substances. The pigments are used so that the coloring extends all the way through the thickness of the finished product.
• Backing material, including webbing for the linoleum, can be made from a wide variety of materials. Natural jute is commonly preferred that is grown as a renewable material in places like India and Bangladesh.
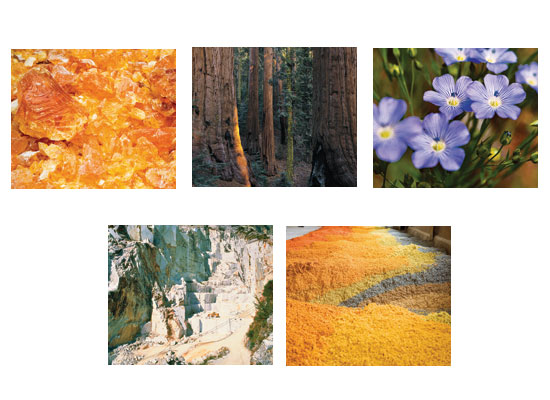
Some of the natural ingredients used in linoleum production include rosin, cork bark, linseed oil from flax, limestone, and environmentally friendly pigments.
Linoleum finished products using these natural ingredients commonly include sheet, tile, and specialty floor coverings that are very well suited to the needs and demands of a healthier, safer indoor environment. In part that is because it is easier to clean and care for than other alternatives. But another important characteristic is its ability to provide natural antimicrobial functions without using any pesticides or biocides. Linoleum is made of natural ingredients that resist microbial growth by their very nature. It has been shown to fight those mutated super bugs including the dreaded CRE bacterium which don't spread effectively on a linoleum surface. Nor will MRSA, C. dif and the other new super bugs. The garden variety bacteria that cause stains and odors won't grow on linoleum either—all due to the natural properties of the ingredients used.

Photo by HMC Architects/Van Dyke Productions; courtesy of Forbo Flooring Systems
Kaiser Fontana Medical Center, Fontana, California
From a green building standpoint, linoleum is 100 percent bio-based and biodegradable.
Independent life-cycle assessments (LCA) have been performed that prove that linoleum is far less harmful to the environment than vinyl and synthetic rubber. Thanks to a formulation that is free of the environmental toxins emitted by vinyl and synthetic rubber flooring, linoleum minimizes threats to current human health and the genetic wellbeing of future generations.
There are some practical benefits from installing linoleum as well. The nature of the product is that pieces seal tightly together meaning that seam welding is not required. By eliminating the cracks between seams that serve as bacterial breeding grounds in vinyl floors, linoleum fights infections while saving time and cost in installation. Linoleum also outperforms vinyl and synthetic rubber in dimensional stability, hygienic protection (when properly installed with net fit seams), and resistance to topical moisture. Linoleum is occupancy-ready at installation and half as expensive to maintain, freeing maintenance staff to create a cleaner, more hospitable healthcare environment. In terms of durability, the 25- to 40-year service life of linoleum far outperforms vinyl or synthetic rubber.
It is important to realize that natural products like linoleum can be used very effectively beyond flooring applications. Linoleum is commonly used as a furniture surface material on nurse's stations, desks, carts, and other permanent surfaces where naturally anti-microbial, anti-static, and easy to clean properties are desired. It can also be used as a cost-effective, highly durable and repairable wall covering or wainscoting for corridors and other areas needing protection. And linoleum bulletin board surfacing material has a multitude of applications. Made from the same natural ingredients as linoleum flooring, it is ideally suited for use as a wall mounted notice board or as a durable finish on furniture, door panels and cupboards.

Photos courtesy of Forbo Flooring Systems
Linoleum is a versatile product suitable for use on wall and desk surfaces where natural antimicrobial qualities are needed or desired.
LEED® and Health
The LEED® rating system as developed by the U.S. Green Building Council (USGBC) has always included significant attention to indoor Environmental Quality (EQ). This system provides a standard for what constitutes a green building but it is important to point out that no single product obtains a LEED credit. Rather, it is the entire building design that is looked at and rated. Nonetheless, natural products like linoleum can readily contribute to a number of credits under the LEED rating system as part of an overall green building design. The LEED 2009 system is in place until the year 2015 which overlaps with LEED version 4 introduced late in 2013. Since buildings are currently being designed under both systems, credits available will vary based on the version used for a particular building.
The Materials and Resources category under LEED v. 4 takes a more holistic approach to defining the green nature of building products compared to LEED 2009. There are still credits for things like Building Re-use and Construction Waste Management, but the rest of the approach focuses on the full life cycle of those products. The key documentation needed to demonstrate performance under this approach is a life cycle assessment (LCA). The results of the LCA are then reported out in an Environmental Product Declaration (EPD). Individual manufacturers or a trade association can prepare specific or generic EPDs for products. The overall intent is to address an emphasis on transparency in the sourcing, ingredient make-up, and manufacturing processes. As called for in LEED v. 4. EPDs are intended to provide Life Cycle Assessment based information and details about the products' environmental aspects thus assisting purchasers and designers in making informed comparisons between products. Properly performed, environmental impacts are assessed throughout the product's life cycle, including raw material extraction, transportation, manufacturing packaging, use, and disposal at the end of a building's useful life.

Photos courtesy of Forbo Flooring Systems
The Children’s Hospital of Pittsburgh used linoleum flooring for an environmentally safe, clean, and attractive design solution that contributed to a sustainable building design.
Several LCA studies have been undertaken on commonly used flooring products. In 1993, Utrecht University's Department of Science, Technology and Society in The Netherlands found that, thanks to the use of natural raw materials, linoleum was clearly the most environmentally compatible floor covering compared to vinyl, wool carpets, and synthetic carpets. The researchers concluded “Comparison shows that linoleum is clearly the best.” A further LCA in 1995 at Chalmers University of Technology in Gothenburg, Sweden was performed in collaboration with the vinyl, chemical and linoleum flooring industries and timber and wooden floor suppliers in Sweden. The conclusion of this LCA states: “Utilizing the most recent data, linoleum has impact values in two of the three assessments similar to those of traditional environmentally compatible pinewood flooring.” In the year 2000, a linoleum only LCA carried out by the Center for Environmental Science, University of Leiden in The Netherlands, concluded that the environmental impact of linoleum was very small. “Potential areas of improvement were identified, and various actions carried through to ensure even more optimal environmental performance.”
When pursuing LEED certification, the USGBC is not asking project design teams to conduct LCAs or to become LCA experts. Instead, a request should be made for an identified manufacture to provide an EPD that discloses the required LCA-based information. In essence, LEED® version 4 will ask product manufacturers to gather the life cycle information on their products and to disclose relevant portions of that information in the standard EPD format. This affects four out of the five MR credits beyond the prerequisites and can contribute towards up to 11 points in the process. In addition to earning points in this revamped MR section of LEED v. 4, an Innovation in Design credit remains available for use of products with SMaRT Certification. This is a separate, independent designation that manufacturers can earn for products that show superior qualities of sustainability. Linoleum is one of the products that has achieved that designation.
LEED v4 has also been updated for some particular building types such as healthcare and schools. LEED for Healthcare in particular recognizes the need to reduce the release of persistent, bio-accumulative, and toxic (PBTs) chemicals in building materials. There are specific credits and points in this version accordingly. LEED for schools also places a high emphasis on IEQ requirements for classroom settings that are focused on creating healthier, safer indoor environments. In both of these settings, the natural product make up of linoleum with its lack of added chemicals will help to insure a desirable outcome.
When selecting or specifying linoleum for any of these settings, there are a number of items to be aware of to assure a fully sustainable design. For example, if an adhesive is required for any installation, be sure it is based on using solvent-free products. Similarly, selecting a floor finish surface that allows for removing dust and loose dirt by dry dust wiping will have the most positive influence on the environmental performance of linoleum. Under normal conditions linoleum floors in healthcare applications do not need significant quantities of disinfectants to be applied. The limited use of water and chemicals contributes very positively to the economic life cycle of the product.
At the end of their life, usually after 25 to 40 years, linoleum floors need to be replaced and disposed of. The two common options include incineration or landfill processing. When burned in an energy-recycling incineration plant, linoleum products produce a residual energy value that is comparable to that of coal (18.6 Mj/kg). It is significant to note that since linoleum does not contain any toxins, its incineration does not release any into the environment the way that other materials can. Incineration of linoleum does not release any “chemicals of concern” because there are none present to begin with or formed by incineration. Further, the amount of CO2 released during incineration is roughly equivalent to that already taken up by the natural raw materials (flax plants, trees and jute plants). Therefore, linoleum is a closed loop system: the energy obtained from incinerating linoleum is roughly equivalent to, or even more than, that which is used in production – and it is toxin free. If incineration is not employed, then linoleum can be safely added to landfill refuse sites, where natural decomposition takes place. Linoleum is fully biodegradable and does not release harmful substances or gases such as chlorine and dioxins. As linoleum's raw materials are provided by nature, and decomposition returns linoleum to nature, this is essentially the ultimate form of recycling. An additional advantage is that the recycling of other floor coverings is usually associated with high levels of energy consumption, with very negative implications in an accurate LCA.
As the previous discussion points out, there is clearly growing recognition and use of EPDs for addressing the environmental impact of building products and materials. Still missing, though, is the attention needed to ecotoxicity and human toxicity in those products. In response, a group of leading architects, building managers and product manufacturers have banded together to create a whole new standard for product hazard reporting that responds more responsibly to concerns of human health and environmental toxicity. The new standard is called the Health Product Declaration (HPD), and it represents a major step forward in product transparency. HPDs build on and incorporate the data from the EPD but goes on to combine it with trustworthy and verifiable measures of ingredients that impact ecotoxicity and human toxicity. As such, it creates a disclosure document that truthfully indicates the toxicity impact of a product on the people who live with it, and the natural environment that it exists within. As envisioned, the HPD will create a single standard that can be used to create an apples-to-apples comparison of products based on their ingredients.
Conclusion
There are no simple answers, but there are solutions that work. The only challenge is to identify those solutions, then gather the organizational and philosophical will power to put them into practice. As a design professional you have the opportunity to make needed changes happen. Every time you select and specify building materials, the means to determine the best and healthiest direction include three actions. First, examine the alternatives with a critical eye. Don't be too quick to embrace a new technology as a magic bullet until the long-term environmental effects are known. The same caveat applies to some well-established solutions like synthetic rubber floor tile, that masquerade as environmentally sustainable when they are actually synthetic products that release lead, mercury and a host of other carcinogens into the environment.
Second, look for the natural payoff. It is important to look at both the short-term cost of installation and the long-term cost of ownership when considering an environmentally friendly solution. The best option is often a product made from natural materials which can provide both the lowest occupancy-ready cost while also delivering the added benefit of low-toxicity, bio-based and biodegradable performance in the future.
Third, don't miss the easy opportunities. Some of the best ideas for improving infection control are also among the simplest. Hands need to be washed, staff members need to wear personal protective equipment and need to be trained in infection control. In design, eliminate areas where harmful bacteria are likely to breed, like the cracks that develop between tiles in a vinyl floor.
We all have a professional interest in protecting the public from indoor toxicity and infection. More importantly, if we are parents, personal caregivers or concerned members of our community there can also be a deeply personal interest. By designing and specifying safe, healthy, indoor environments, we help ensure the well-being of the public, our children, and grandchildren for generations to come.
References
1. The Biocidal Products Regulation (EU 528/2012). For more information: http://echa.europa.eu/regulations/biocidal-products-regulation
2. “Chemicals and Our Health: Why Recent Science is a Call to Action”, a report published by the Safer Chemicals Healthy Families coalition.
3. “The Future of Fabric – Health Care,” published by the Healthy Building Network, October 2007 in conjunction with Health Care Without Harm's Research Collaborative.
4. http://www.chicagotribune.com/chi-infectiousdiseases-specialpackage,0,2681727.special, http://www.chicagotribune.com/news/chi-0207210272jul21,0,2177158.story
5. Sathyanarayana, S. (2008) Phthalates and children's health. Current Problems In Adolescent Health Care, 38, 34-39. doi:10.1016/j.cppeds.2007.11.001
6. “Toxic Chemicals in Building Materials; An Overview for Health Care Organizations” Kaiser Permanent and the Healthy Building Network/Healthcare Without Harm, May, 2008
7. Pharos Product Category Descriptions – Resilient Flooring, http://www.pharosproject.net/product_category/show/id/3
8. America's Children and the Environment, U.S. Environmental Protection Agency, 2008. http://www.epa.gov/ace/
9. Holly L. Howe, et al., “Annual Report to the Nation on the Status of Cancer (1973 through 1998), Featuring Cancers with Recent Increasing Trends,” Journal of the National Cancer Institute, 93, no. 11 (June 2001): 824–42. http://jnci.oxfordjournals.org/content/93/11/824.full.pdf?origin=publication_detail
10. Janet Gray, ed, State of the Evidence: The Connection Between Breast Cancer and the Environment (San Francisco: Breast Cancer Fund, 2008).
11. Tracey J. Woodruff , et al., “Trends in Environmentally Related Childhood Illnesses,” Pediatrics, 113, no. 4 (April 2004): 1133-1140.
12. Jeanne E. Moorman, et al., “National Surveillance for Asthma, United States 1980–2004,”Centers for Disease Control and Prevention, www.cdc.gov/mmwr/preview/mmwrhtml/ss5608a1.htm (November 1, 2009).
13. Anjani Chandra and Elizabeth Hervey Stephen, “Impaired Fecundity in the United States:1982-1995,” Family Planning Perspectives, 30, no 1, (1998): 34-42.
14. Anjani Chandra, et al., “Fertility, Family Planning and Reproductive Health of US Women: Data from the 2002 National Survey of Family Growth,” Vital and Health Statistics, 23, no. 25 (2005).
15. Kate Brett, “Fecundity in 2002 National Survey of Family Growth Women 15–24 Years of Age” (personal communication), Hyattsville, MD, National Center for Health Statistics (2008) http://www.womensvoices.org/issues/reports/the-health-case-executive-summary/
16. Leonard J. Paulozzi, “International Trends in Rates of Hypospadias and Cryptorchidism,” Environmental Health Perspectives, 107, no. 4, (1999): 297-302.
17. National Institute of Mental Health, “NIMH's Response to New Autism Prevalence Estimate,” http://www.nimh.nih.gov/about/updates/2009/nimhs-response-to-new-autism-prevalence-estimate.shtml
18. Scientific American “The Baffling Link Between Autism and Vinyl Flooring,” Marla Cone, Environmental Health News 2009
19. Linoleum Life Cycle Assessment: www.leidenuniv.nl/cml/ssp/publications/lcalinoleum.pdf
20. HPD Open Standard developed by Health Product Declaration Collaborative www.hpdcollaborative.org
Forbo Flooring Systems has been creating better environments with its beautiful, durable flooring products for over 100 years. Forbo is committed to complete transparency in its products and the industry, and has included its
eco-toxicity and human health and toxicity impacts in the publication of its EPDs in support of full disclosure and transparency. |