Meeting New Water Quality Mandates in Health-Care Settings
New national standards target reducing the risk of Legionnaires’ disease
![]() Continuing Education
Continuing Education
Use the following learning objectives to focus your study while reading this month’s Continuing Education article.
Learning Objectives - After reading this article, you will be able to:
- Identify and recognize the conditions that contribute to the development and growth of legionella in health-care facilities.
- Investigate the requirements of ASHRAE 188 and the new DHHS policy memorandum related to water quality in health-care settings to reduce the risk of Legionnaires’ disease.
- Assess the potential ways to address legionella in water supply, distribution, and drainage systems in health care.
- Specify products that can contribute to compliance with water quality requirements contained in the DHHS policy memorandum and ASHRAE 188.
Hospitals and other health-care facilities in general require water to operate, and usually a lot of it. It is used not only in patient room sinks, showers, and toilets, but also in staff sink/scrub areas, wellness rehab areas, food service centers, public restrooms, and laboratories. Additionally, water drives many of the mechanical systems in a facility, including HVAC systems, fire protection, and domestic water systems, both hot and cold. All of this water is intended for good outcomes but can also be the primary cause of concern for unintended consequences since water can be a prime breeding ground for bacteria and disease if not managed properly. Waterborne pathogens can be a threat not only to patients but also to staff, visitors, and other people who come in contact with liquid water, vapor, or airborne spray in a health-care setting. One of the most troubling of those pathogens is legionella bacteria, which is the cause of Legionnaires’ disease (abbreviated LD or also called Legionellosis), which is a type of pneumonia that can lead to severe disabilities or even death. Its name comes from one of the first and most public discoveries of the condition, which occurred at a 1976 convention of the American Legion where a number of attendees (i.e., Legionnaires) became sick and/or died. The cause was ultimately traced to infected airborne moisture in the HVAC system of the hotel. Since then, the Centers for Disease Control (CDC) have investigated the condition at great length and tracked anywhere from 8,000 to 18,000 cases per year of people that have become infected in the United States. Obviously, they don’t all make the news, but the concern is real and significant in health-care settings, so much so that new standards and guidelines are now in place that are applicable to designers, facility managers, and health-care executives. This course will look at some of the concerns over LD, the requirements of standards related to controlling or eliminating cases and outbreaks, and some of the fundamental design implications related to water-based systems in health-care settings.

All images courtesy of Watts, except as noted
Health-care facilities treat patients who suffer from disease, but new standards seek to be sure they don’t also cause infectious breakouts caused by water-borne bacteria, such as Legionnaires’ disease.
Health Care and Legionella
Those tasked with managing and operating a successful health-care facility typically focus on achieving some fundamental goals. These can include safety for their patients, employees, and the public, providing comfort for those within the facility, and appropriate efficiency in operations. Ultimately, the goal of everyone who works or visits a health-care facility is the overall satisfaction of the patient. When it comes to treating patients with Legionnaires’ disease, all of these goals apply, so it is worth understanding a few fundamentals and statistics about the disease:
- Legionnaires’ disease doesn’t spread from person to person. Instead, the bacteria spreads through mist, such as from cooling towers, evaporative condensers, showers and faucets, whirlpool spas, decorative fountains and misters (source: ASHRAE 188).
- Those at most risk include persons who are at least 50 years old, smokers, or those with underlying medical conditions such as chronic lung disease or immunosuppression (source: Mayo Clinic and others).
- Many people exposed to legionella bacteria don’t develop symptoms, but those who do may experience cough, fever, chills, shortness of breath, muscle aches, headaches, and diarrhea (source: Mayo Clinic and others).
- LD can be treated with antibiotics, such as azithromycin or ciprofloxacin, assuming it is diagnosed properly and in time for the antibiotics to help (source: Mayo Clinic and others).
- Cases of LD reported annually in the United States from 2000–2009 increased by 217 percent; measured from 2000–2014, the increase is 400 percent (source: CDC).
- The number of direct health-care dollars it costs in the United States to treat a single case of Legionella is $34,000 (source: CDC).
- The cost to the health-care system for hospitalizations for three common waterborne diseases is $539 million annually, with Legionnaires’ disease being the largest cost (source: CDC). In addition, if a person acquires Legionnaires’disease while a patient at the hospital, the hospital may not get reimbursed for expenses related to his/her care.


Legionella bacteria in water systems can spread to people through the air causing a severe type of pneumonia called Legionnaires’ disease, which has been reported in an increasing number of cases since the year 2000.
While LD is clearly a potential source of income for care in hospitals, if the infection is contracted while someone is in a health-care facility, it can have potentially dire consequences on the continued operation of the facility.
Consider these statistics:
- The CDC has investigated building-associated outbreaks of LD and determined that the most common places for contracting the disease are hospitals, long-term care facilities, and hotels. In these types of buildings, the sources for spreading water droplets contaminated with legionella can include things like showers and faucets of building plumbing systems, cooling towers, hot tubs, decorative fountains, and aerosolizing water features (source: ASHRAE).
- The range of reported jury awards and settlements related directly to LD is $255,000 to $5.2 million. (Reports of settlements are rare, as most agreements include stipulations that payout amounts remain confidential.) The serious personal injury or death caused by this disease makes proof of extensive compensatory damages simple (source: Claims Management).
- The largest dollar jury award (so far) for LD plus gross negligence and other failures that resulted in long-term disability and severe debilitation is $193 million. The case was not fatal (source: Claims Management).
It is not surprising then that hospital executives and facilities management teams are not only aware of this potential liability but are actively working to prevent legionella outbreaks. It is also not surprising that national standards have recently emerged to provide guidance not only to hospital personnel but also to design professionals on how to address this potential threat.
ASHRAE Standards
The American Society for Heating, Refrigeration, and Air-Conditioning Engineers (ASHRAE) has taken note of the connection between water-based mechanical and plumbing systems in buildings and legionella bacteria growth. After reviewing the concerns and conditions, it first published a guideline in the year 2000 titled Guideline 12-2000 – Minimizing the Risk of Legionellosis Associated with Building Water Systems. It has continued to review the issue and in 2015 published an updated ANSI/ASHRAE Standard 188: Legionellosis: Risk Management for Building Water Systems. This standard, which it suggests “is essential for anyone involved in design, construction, installation, commissioning, operation, maintenance, and service of centralized building water systems and components,” establishes minimum risk management requirements for building water systems to combat the legionella bacteria. It not only includes a description of the environmental conditions that promote the growth of legionella, but it also outlines action plans for managing and monitoring those conditions. Additionally, there are informative annexes and a bibliography that contain suggestions, recommendations, and references for additional guidance.

ASHRAE has been heavily involved in the creation of guidelines and standards to reduce the risk of legionella outbreaks in buildings since the year 2000.
ASHRAE 188 begins by pointing out that while legionella bacteria occur naturally in freshwater environments, it becomes a health concern when it grows in building water systems that are not adequately maintained. It also recognizes that the mere presence of legionella in a water system or device is not sufficient to cause disease. Rather, to cause illness, the bacteria must ultimately be inhaled or aspirated into the lungs of a susceptible person. Nonetheless, there is enough incidence of that happening to warrant a concerted effort to prevent legionella growth in buildings.
A key focus of ASHRAE 188 is to assist designers and building operators in developing a specific water management program for the systems that exist in their buildings or campuses. It recognizes that design, good operations, and maintenance procedures that prevent growth and spread of legionella are regarded as the best methods of preventing disease. In fact, CDC investigations of outbreaks show that 9 out of 10, or nearly all of them, were caused by problems preventable with more effective water management. Therefore, developing a water management program with the recommended practices can definitely reduce the chance of bacteria colonization, amplification, and dissemination to people. Of course, it cannot guarantee that a system or individual component will be totally free of legionella, but it should be able to keep it down within acceptable limits.

ASHRAE standard 188 describes seven steps that are involved in an ongoing water management program for commercial and institutional buildings, including health-care facilities of all types.
Creation of a water management program under ASHRAE 188 includes a seven-step process as follows:
- Program team: The persons responsible for the development and implementation of the program need to be identified. This will necessarily include a design professional familiar with the design and operation of all of the water systems in the facility. Suggested team members include infection prevention personnel, a legionella expert who could be a consultant or equipment manufacturer, upper management personnel with decision-making authority, and facility management.
- Water systems description and flow diagrams: For existing buildings, a complete survey and documentation of the water systems by a design professional are called for using the process described in the standard. For new buildings, all potable and nonpotable water sources need to be assembled for the building(s) and the site, including schematics of all water systems.
- Analysis of building water systems: A professional evaluation needs to take place to determine where hazardous conditions may occur that could promote the growth of water-borne bacteria.
- Control measures: A determination needs to be made of locations where control measures must be applied and maintained in order to stay within established control limits of any legionella bacteria growth. Once determined, the control measures need to be implemented accordingly.
- Monitoring and corrective actions: Procedures for regular and routine monitoring of the effectiveness of the control measures need to be developed and carried out. If the system is not operating with established limits, then corrective actions must be taken to restore effectiveness.
- Confirmation: Additional procedures need to be in place first to verify that the program is being implemented as designed and second to validate that the hazardous conditions throughout the building water systems are being controlled.
- Documentation: All activities of the program need to have documentation and communication procedures in place and carried out.
Overall, the key is to bring the right people together to follow the process and develop specific procedures for a particular facility to adopt and implement. Within this framework, ASHRAE 188 articulates the requirements for building surveys and building water systems in detail to identify specific criteria that need to be incorporated. There is also a specific section covering requirements for designing building water systems and one specific to health-care facilities. Like all standards, ASHRAE 188 is a voluntary consensus standard that may or may not be adopted into local plumbing codes. If it is, enforcement is most likely performed by the local authority having jurisdiction. Otherwise it may be adopted by a local health-care organization or used to support certification or accreditation of the facility.
Medicare/Medicaid and Legionella
The Department of Health & Human Services (DHHS) Centers for Medicare and Medicaid Services (CMS) is the arm of the federal government that provides funding and oversight for facilities and care providers administering to patients using Medicare or Medicaid insurance. In addition to being an important source of income for health-care facilities, CMS oversees requirements for long term health-care facilities. In June of 2017, they developed and released a new policy memorandum titled “Requirement to Reduce Legionella Risk in Healthcare Facility Water Systems to Prevent Cases and Outbreaks of Legionnaires’ Disease (LD).” This policy memorandum applies to hospitals, critical access hospitals (CAHs), and long-term care (LTC) but is also intended to provide general awareness for all health-care organizations.
Under this policy memorandum, CMS expects Medicare certified health-care facilities to have water management policies, management teams, and procedures in place to reduce the risk of growth and spread of Legionella and other opportunistic pathogens in building water systems. The basis for these policies and procedures is ASHRAE Standard 188, and in 2016, the CDC and its partners developed a toolkit to facilitate implementation by facilities.1 This toolkit describes the environmental, clinical, and epidemiologic considerations for health-care facilities related to legionella. It also provides some suggested logistics of establishing a water management team, conducting surveys, and developing/implementing a water management program per ASHRAE 188. It includes control measures such as physical controls, temperature management, disinfectant level control, visual inspections, and environmental testing for pathogens.

The Center for Disease Control (CDC) has published a water management toolkit resource for building designers, managers, and owners to use based heavily on ASHRAE 188.
Of particular note to health-care executives, facilities are expected to comply with the CMS requirements to protect the health and safety of its patients. Those facilities deemed unable to demonstrate measures to minimize the risk of LD are at risk of citation for noncompliance with the CMS Conditions of Participation. The CMS policy memorandum indicates quite clearly that “Accrediting organizations will be surveying health-care facilities deemed to participate in Medicare for compliance with the requirements listed in this memorandum, as well, and will cite noncompliance accordingly”. Based on this, it is expected that all health-care facilities will have a renewed interest in establishing and carrying out a full water management program based on ASHRAE 188 and the CMS policy.
Water Systems and LD in Health-care Facilities
With an understanding of the nature of the issues and the requirements of the standards, let’s turn our attention to the specific parts of a water system in health-care facilities that need to be addressed. Most commonly, LD outbreaks are linked to environmental reservoirs in large or complex water systems, including those found in health-care facilities such as hospitals and long-term care facilities. When water is moved or sprayed into the air, such as in showerheads, cooling towers, hot tubs, and decorative fountains, then transmission of the legionella bacteria to humans is possible. Further, legionella can grow in parts of building water systems that are continually wet and within a temperature range suitable for growth. The ideal range of temperature for such growth is 95 to 115 degrees Fahrenheit, but the bacteria is known to grow and be active anywhere between 68 to 122 degrees Fahrenheit. Below 68 degrees, legionella bacteria can survive but are dormant, while above 122 degrees they can survive but do not multiply. The bacteria will die slowly when temperatures in the water reach 131 degrees Fahrenheit and rapidly between 158 to 176 degrees.

Legionella bacteria is very sensitive to temperature. It can go dormant at low temperatures, thrive in normal building temperatures, and be killed at higher temperatures.
Since a building water system contains many different subsystems and components, we will review some of the major ones in the following sections with a discussion of the relevant approaches to identifying legionella hazards and control methods.
Water Supply Components
Most health-care facilities rely on a public or municipal water source that has likely been treated in a centralized plant and piped through public water supply lines. The water leaving the plant has certainly been tested and maintained to prescriptive levels for potability and human health, but there is no guarantee that its trip through an aging piping system will keep it that way. Water line breaks, outdated joint connections, and other conditions all have the potential for contaminating municipal water delivered to a building. Therefore several water supply components deserve particular attention.
- Backflow preventers: Among the common approaches to protecting water quality in a water supply system, the use of backflow preventers is typical. Backflow systems are essentially a series of plumbing control valves that prevent the reverse flow of polluted water from entering into the potable water supply due to back-siphonage and/or backpressure. Some municipal water systems will require backflow systems, particularly on large water users such as health-care facilities, since it is in the interest of public safety and health to do so, especially if there is any chance of infectious bacteria entering the water system. Therefore, including backflow preventers can be part of a control measure in a water management program. When selecting back flow preventers, there are choices to consider. Stainless steel versions are available as basic or mid-tier products with some limited options. More robust and durable choices include ductile iron valves, some with epoxy-coated paint on the exterior and designs for continuous or heavy usage.
- Pressure reduction: One of the things that can alter the performance of any water system is the water operating pressure. Water coming in from a municipal system may be affected by other buildings as well as the level of demand in a health-care building. Either way, if the pressure is too high, some parts of the building water system may not work well or can be damaged. If the pressure is too low, then water may not flow as intended and may lead to conditions that are unwanted. The remedy is to install a valve to regulate the water pressure in the building.

Water pressure reducing valves (WPRV) can help control water pressure throughout a facility. A single regulator installation, shown here, is the most typical installation configuration. It is recommended where incoming pressure is less than 200 psi and when the reduction ratio is less than 3:1.
There are two fundamental choices in this regard. The first is a conventional water pressure reducing valve (WPRV), which reduces fluctuating high inlet pressure to a constant lower outlet pressure. Such WPRVs typically have a broad range of flow potential and can be fully adjustable. For example, a municipal water system that is providing water in the 80 to 100 psi range could be regulated to a constant 50 psi with an appropriately sized and set WPRV. Further, smaller WPRVs could be located within an overall system to be set for different settings to suit the optimal pressure needs of different parts of a health-care facility. The second option is to use an automatic control valve (ACV) that provides the same function but is designed and constructed differently. The primary operating difference between an ACV and a WPRV is the flow rate in gallons per minute (GPM) compared to the pressure in the system. Using a WPRV, the pressure will decrease as the flow increases. However, with an ACV, the pressure can remain fairly constant even as flow rates reach up to about 250 GPM.

Automatic control valves help maintain water flow rates unlike direct acting pressure reducing valves, which typically reduce pressure as flow rates increase.
One item related to flow rates is the current code requirement for many faucets and fixtures to operate in low-flow conditions for the purpose of conserving water. This is good for water use but can cause water to pool or sit in systems longer than otherwise desired to control legionella growth. Therefore, water pressure control valves and low-flow fixtures need to be an integral part of the water management program with regular monitoring, maintenance, and reporting.
- Water-disinfecting systems: With any uncertainty over the quality of the water entering a building, many health-care facilities are being proactive and using a centralized system to at least filter if not fully disinfect the incoming water. Of particular relevance is a centralized ultraviolet (UV) disinfection system that is highly effective at providing protection against microbiological contamination in water. These systems are attractive not only because they can be very effective at killing microorganisms, such as legionella bacteria, but also because they are fairly simple to use and operate. Connected to a power source, they produce the UV light that is projected onto the incoming water without the need for any chemicals to be handled or added to the water. For large systems, they are commonly completely enclosed for safety to prevent any accidental UV exposure to people. They also typically have sensors indicating their use and performance levels and can be specified to operate efficiently by only turning on when there is actual water flow in the supply line.
- Anti-scale systems: Scale is related to potable, clean drinking water that has a high mineral content and is referred to as “hard.” Over time, the minerals can attach to the metallic surfaces of a water system and start to build up. The resulting scale often becomes encrusted on the internal moving parts of valves and components, affecting their intended purpose and potentially causing safety failures. In a boiler or hot water tank, heating elements can become coated with scale, reducing system efficiency and safety. In pipes and other components, it can restrict water flow and create potential breeding grounds for bacteria. The solution here is an anti-scale system, also sometimes referred to as a water softening system. A conventional system typically relies on the use of salts that need to be constantly replenished into the system as water flows through it. An alternative is to use a template-assisted crystalline (TAC) system that eliminates the need for salt, takes up less square footage than a water softening system, and is generally regarded as much more economical with similar results.
Of course, there are other ways to disinfect water systems too. Some of the more traditional methods involve copper solutions, chlorine, and other chemical treatments. Those can be evaluated for how well they may suit the needs of a particular building but should be compared to UV systems for effectiveness, cost, and ease of operation. There is also the option of using high-temperature sanitization. Some water-heating control systems allow operators to set temperature and run times to purge the water system at 158 degrees Fahrenheit or higher, which is the rapid-kill temperature zone for legionella bacteria. This regular and routine sanitation is a legitimate part of an overall water management system program.

TAC water-softening systems used to fight scale buildup are more efficient without requiring salts and take up noticeably less square footage compared to conventional water softeners.
Addressing each of these water quality issues at the source is the best way to assure that the water entering a facility does not have the potential to introduce or contribute to water-borne bacteria development and growth.
Water for HVAC Systems
Some of the water used in buildings is not for direct contact with people but is used instead for heating and cooling systems. Hydronic heating systems with boilers, for example, often use water storage tanks to balance out the water requirements of the system. That water could be a breeding source of bacteria if the temperature conditions and other circumstances are favorable. Of more concern are cooling systems, particularly those that use water cooled by evaporation into the surrounding air. This can be occurring on a large scale, such as a centralized cooling tower that cools down the water and recirculates it into the building air-conditioning system. It can also happen on a smaller scale, such as packaged terminal air-conditioners (PTAC units) or piped systems with local heat exchangers that are common in many health-care settings since they offer individual temperature control in each room. It was in units like these that the Legionnaires’ disease was first found to be growing and getting blown into rooms. All of these systems need to be part of a water management program and will likely require regular checking and monitoring of their operation to be sure that no water is escaping into the air or being created by condensation and allowing bacteria to form.
Water Distribution Components
Once the water is in the facility, it needs to be distributed appropriately for use on demand. Depending on the size and nature of the facility, that may prove to be rather complex, which is why the schematic flow diagram of a water system is important as part of a water management program. We will look at some of the common components of a distribution system here.
- Cold water storage tanks: Some facilities with high water flow requirements will use an on-site water storage tank to buffer the demand with the usage. That is an appropriate and time-honored method, but keep in mind that such tanks can also be a breeding ground for legionella and other bacteria. Therefore, the temperature of the water should ideally be kept below 68 degrees Fahrenheit to keep legionella dormant without the risk of activity.
- Hot water heaters and tanks: Water in a hot water tank is generally kept at an appropriate temperature for warm or hot water use in a building at around 110 to 120 degrees Fahrenheit. Unfortunately, that temperature can also be in the ideal range for legionella bacteria to grow and thrive. If the temperature hasn’t been appropriately raised to the ASHRAE-recommended 140 degrees Fahrenheit to kill legionella within 30 minutes, then there is the risk of bacteria growth. This will need to be addressed and monitored or the water tanks will need to routinely heat up to these kill-range temperatures to protect against any growth or spread of legionella.
- Mixing valves: While heating water to the rapid-kill range is one of the most effective and reliable control measures for dealing with legionella, it is not necessarily the best temperature for heated water to be used by people. On average, any water that is above 106 degrees Fahrenheit will cause scalding and pain in humans, while water that is 140 degrees Fahrenheit can cause third-degree burns in a matter of seconds. This is why plumbing codes limit the maximum temperature exiting a fixture at 120 degrees with the expectation that people can readily control the mix of cold and hot water at the faucet to meet their needs. However, there are plenty of things that can change the water temperature coming out of those faucets. For example, it is common for a health-care building to use a recirculating system that pumps hot water uniformly through the hot water piping to prevent long wait times for heated water at a faucet, etc. However, things like pressure fluctuations can cause hot and cold water to move less predictably through the system, while valves in the system could malfunction or fail. Mixing valves helps compensate for those discrepancies and deliver a more predictable water temperature output.
Clearly, it’s important to meet both the needs of killing legionella with higher-temperature water and the human requirements of a lower, useful temperature. The solution is found in the use of tempering valves or mixing valves that blend hot water (generated and stored at temperatures high enough to kill bacteria) with cold water in a controlled manner. This ensures constant, safe outlet temperatures while minimizing the occurrences of both scalding and legionella.
When looking at mixing valve systems, there are two fundamental types. A point-of-source (POS) system locates valves at or near the water-heating source and typically has a higher capacity for controlled temperature water. A point-of-use (POU) system uses multiple, smaller mixing valves at or near plumbing fixtures, such as showers, lavatories, whirlpools, and emergency fixtures. Both types are common and have a range of standards issued by the American Society of Sanitary Engineers (ASSE) relevant to particular usage.

Thermostatic mixing valves can be installed and used as a point-of-source system (left) or as a point-of-use system (right).
- Digital mixing systems: Beyond purely mechanical mixing valves, computerized digital mixing systems are also available that are considered a smarter and safer way to deliver mixed water throughout a health-care facility. In this type of system, intelligent control modules and electronically actuated valves are used to allow faster and more accurate response to constant changes in the mixed water delivery demands, often anticipating system changes before they occur. Further, digital water mixing and recirculation solutions can be integrated into a building automation system to allow facility managers compete control of and visibility into their domestic hot-water delivery.
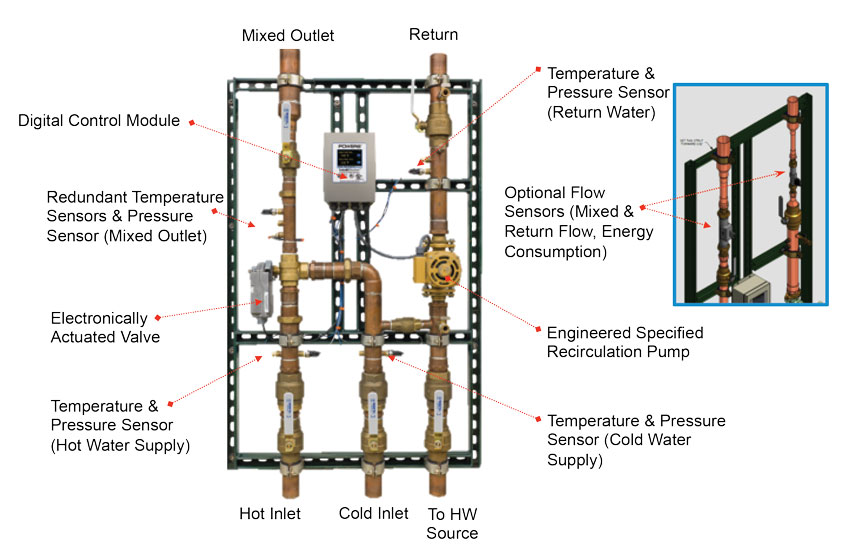
A digitally controlled temperature-mixing system provides the most accurate control of water temperature in buildings.
As a point-of-source system, a digital mixing and recirculation station can provide precise control of hot water delivery within 2 degrees of the set point, surpassing industry standards for mechanical systems. Further, it eliminates temperature creep within the system, thus eliminating the need for balancing valves. All of this means that it can more precisely be controlled to mitigate legionella growth in the heated water. In particular, a sanitization or disinfectant mode can be triggered to briefly raise the temperature above 158 degrees Fahrenheit to induce a “rapid kill” and purge all legionella bacteria. At the same time, the digital mixing system can control temperatures leading to faucets, showers, etc. to reduce the risk of scalding in the mixed water. If combined with separate point-of-use protection, then it allows for continuous elevated circulation temperatures to prevent legionella per ASHRAE and CDC guidelines. Concurrently, the digital system can control the circulation pump to prevent stagnant conditions or maximize flow rates. Finally, since most large facilities use some type of building automation system, a digital mixing system can be linked to the larger system to communicate and control temperature, pressure, flow, and energy consumption as part of an overall operations and maintenance plan. It also makes documentation and verification more straightforward in a water management program as called for in ASHRAE 188. From a specification standpoint, most of these systems are easy to install since they typically come pre-piped, pre-wired, and tested, allowing them to carry a warranty from the manufacturer for up to five years.
- Pipes: The pipes throughout the premise plumbing system must be considered. Material, age and design can affect pipes ability to be bacterial resistant. Besides the standard shower channels and floor drains for hospital applications, there has been an increased demand for stainless steel piping that is replacing cast iron stacks in facilities due to the extreme corrosion that is occurring within a three to four year period with the existing cast iron.
One potential cause for the increased corrosion is lack of water volume.
Cast iron corrosion could be attributed to the increase in low water faucets, toilets, and urinals used at hospitals. When the cast iron was initially installed, the required flow rate of wastewater was typically set due to Manning’s Formula for gravity waste piping. Based on the number of fixtures and toilets and amount of flow each fixture generates per flush or operation pipe diameter is determined.
The change to low water fixtures drastically decreased the amount of water going through the pipes which can lead to the cast iron piping being unable to self-clean and flush all of the solids in the wastewater system. This deposit of solids becomes a food source for bacteria and allows them to mitigate and breed.
Off gas of hydrogen sulfide also occurs that creates sulfuric acid once it rises to the top of the inside wall of the cast iron piping. The result is longitudinal splitting and crowning corrosion of the cast iron and pipe leakage/failure inside the hospitals.
Stainless steel piping has the most resistance to biofilm formation compared to other materials on the market. Blucher piping is 316 stainless steel with 18% chromium content that is pickled and passivated during manufacturing. This means that the chromium in the stainless reacts with oxygen in the wastewater to “self-heal” and replenish the chromium oxide coating on the piping. This increases the longevity of the piping to an estimated 75+ years due to its inability to allow corrosion of the pipe. It is this chromium oxide coating that prevents/reduces the ability for bacteria in the wastewater to find microfractures in the piping to breed, harbor, and mitigate.
Hospitals are capitalizing on decreased labor for the renovation and installation with Blucher piping. Interest in the push-fit hub and spigot designed piping from hospital maintenance managers continues to significantly increase because it reduces the amount of plumbers needed for renovation (stick of 4” diameter 10’ Blucher stainless weighs roughly 16lbs compared to stick of 4” diameter 10’ cast iron that weighs roughly 76lbs). The push-fit installation eliminates any welding and decreases install time compared to no hub cast iron installations while still maintaining 7psi rating with standard gasket, 15-30 psi rating with joint clamp, and 44 psi rating with joint clamp and projects at the connection.
Hospitals cannot afford to have systems shut down. With the decrease in labor associated with installation of stainless-steel push-fit piping, hospitals decrease the time they have to shut down rooms/floors for the renovation. Savings has been recorded roughly $5000-$10,000 in decreased shut down time per renovation.
Double containment piping is being used by hospitals for the piping going over and near kitchens and other high-risk areas such as operating rooms. The double containment system is unique because it is simply “pipe in pipe” so you are installing it the same way as standard piping, just building it with a diameter larger pipe “sleeve” during installation.
- Valves, and fittings: If all of the measures described thus far are followed, then the water flowing through the distribution piping, valves, and fittings should be fairly safe, but that doesn’t mean they don’t need to be checked, inspected, and verified as part of the water management program. Valves of all types in particular can be a concern, so working closely with manufacturers to identify and specify those that are most suitable for preventing problems and growth is appropriate.
- Faucets and wash stations: The point-of-use fixtures are where people come in contact with water throughout the health-care facility. The primary concern is that a biofilm of bacteria can start to form on edges or within components of a faucet or wash station. If that bacteria is allowed to build up in things such as aerators or faucet flow restrictors, then it could either build up and grow, or worse, be sprayed into the air and cause illness. That means such components need to be checked, cleaned, or replaced regularly. A related concern is the location of wash fixtures and the potential for water splashing onto either people or equipment used to treat patients. Separating sinks and other water stations from medication dosing areas, and equipment is one way to help minimize the possibility of cross contamination. Using splash guards around sinks and scrub areas can also be effective in some areas.

The points where people come into contact with water in a facility is where legionella and other bacteria can be released from a biofilm buildup or sprayed into the air and breathed in.
- Showerheads and hoses: Showers and hoses pose additional concerns since biofilm formation can be particularly problematic here. Handheld showers are common in health-care facilities, but the hose portion can hold water between uses, and the showerhead itself can remain warm and moist, allowing bacteria growth. The recommendations here include allowing the hoses to hang down and drain after each use. It is also prudent to replace handheld showers periodically.
Drainage Systems
The final part of a water management program includes attention to the drainage systems in a building. Since virtually all of the water that flows through a facility is used and then drained away (except for drinking or evaporation), the drainage system needs to be free of legionella and other bacteria as well. This means that water must be freely draining with no opportunity for stagnation or biofilm formation here either.
When it comes to drainage piping, nonporous materials are preferred in health-care facilities. Porous materials, such as some metals and plastics, can become unintended breeding grounds for bacteria growth. Significantly lower growth of bacteria has been found on stainless steel, making it the ideal solution for applications where hygiene is a concern, particularly in kitchens and food service areas of health-care facilities.
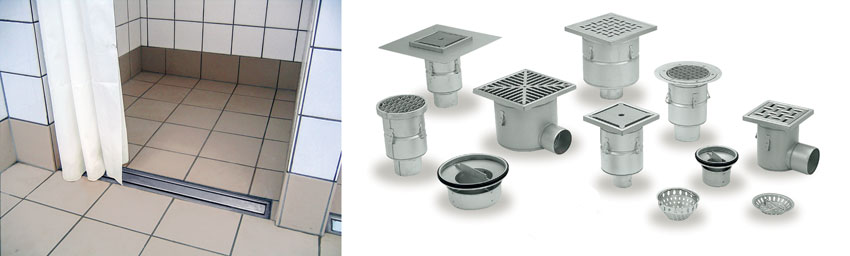
Stainless steel drainage components remain cleaner and less likely to contribute to bacteria growth.
Design Considerations
Plumbing systems can be complicated, especially within a hospital. A majority of hospitals are older structures that have been added on to and renovated multiple times. This increases the complexity of water systems. Some design methods include continuous recirculation of domestic hot water; high water temperature is maintained throughout the main waterway, with tempering valves at all points of use.
Yet, there are still challenges. Consider first that many large facility domestic water systems can contain many thousands of gallons of water (U.S. hospitals are water hogs, using an average of 570 gallons of water per staffed bed). That’s a lot of water. Consider, too, that as water moves away from heat sources where temperatures may be sufficient to prevent germ growth, those large pipelines may cool domestic hot water to ideal temperature ranges for waterborne pathogens.
Consider, too, ubiquitous biofilm within those piped waterways. As microbes grow, they attach themselves to wetted surfaces in water distribution systems. They protect themselves from disinfecting agents, and heat, by forming biofilm. A biofilm contains a group of bacteria enveloped within a polymeric slime that ensures adhesion to the pipe surface – and a nice, soft place for resilient microbes to grow and prosper. The biofilm also contains the food for bacterial growth, adding substantially to the importance of this challenge.
Even water in new facilities has this risk. Consider how long water has been in the building prior to opening the building for operation. Typically, many months; there it sits, becoming stagnant – a perfect home for biofilm buildup and bacterial growth. Sadly, many hospitals have opened only to be confronted with numerous legionella cases, the source being the water that was introduced to the piped systems long before the first patient walked in the door. Proper disinfection and flushing must happen to help combat this problem.
Some of the major design considerations for legionella risk mitigation include:
- Continual circulation
- Elimination of dead legs
- Maintaining a high-water temperature throughout the system
- Utilizing solutions from POE to POU
Conclusion
Outbreaks of illness, particularly Legionnaires’ disease, can be dramatically reduced or potentially eliminated in health-care settings if proper attention is paid to the important aspects of water management. The protocol and requirements of ASHRAE 188 are recognized by facility managers and governmental bodies as the best place to start since it is based around a comprehensive and continuous water management program. In fact, continued accreditation and funding for a facility under Medicare and Medicaid may depend on it. Reviewing and addressing all components and opportunities in the supply, distribution, and drainage portions of a building water system is needed to produce a proper program. Ultimately, it is the collaboration of design professionals, facility managers, equipment suppliers, and others that allow for the successful development and ongoing monitoring of an effective water management program.
End Notes
1“Legionella (Legionnaires’ Disease and Pontiac Fever).” Centers for Disease Control and Prevention. 2 June 2017. Web. 14 August 2017. www.cdc.gov/legionella/maintenance/wmp-toolkit.html
Peter J. Arsenault, FAIA, NCARB, LEED AP, is a practicing architect, green building consultant, continuing education presenter, and prolific author engaged nationwide in advancing building performance through better design.
www.linkedin.com/in/pjaarch
|
|
Watts is a global leader in the design and manufacture of innovative water solutions for residential, commercial, and institutional environments. Products include an extensive line of flow control, filtration, and treatment products for water quality and residential plumbing and heating. Founded in 1874, Watts is headquartered in North Andover, Massachusetts. www.watts.com |